

Overcoming therapeutic resistance in glioblastoma: the way forward
- PMID: 28145904
- PMCID: PMC5272196
- DOI: 10.1172/JCI89587
Overcoming therapeutic resistance in glioblastoma: the way forward
Abstract
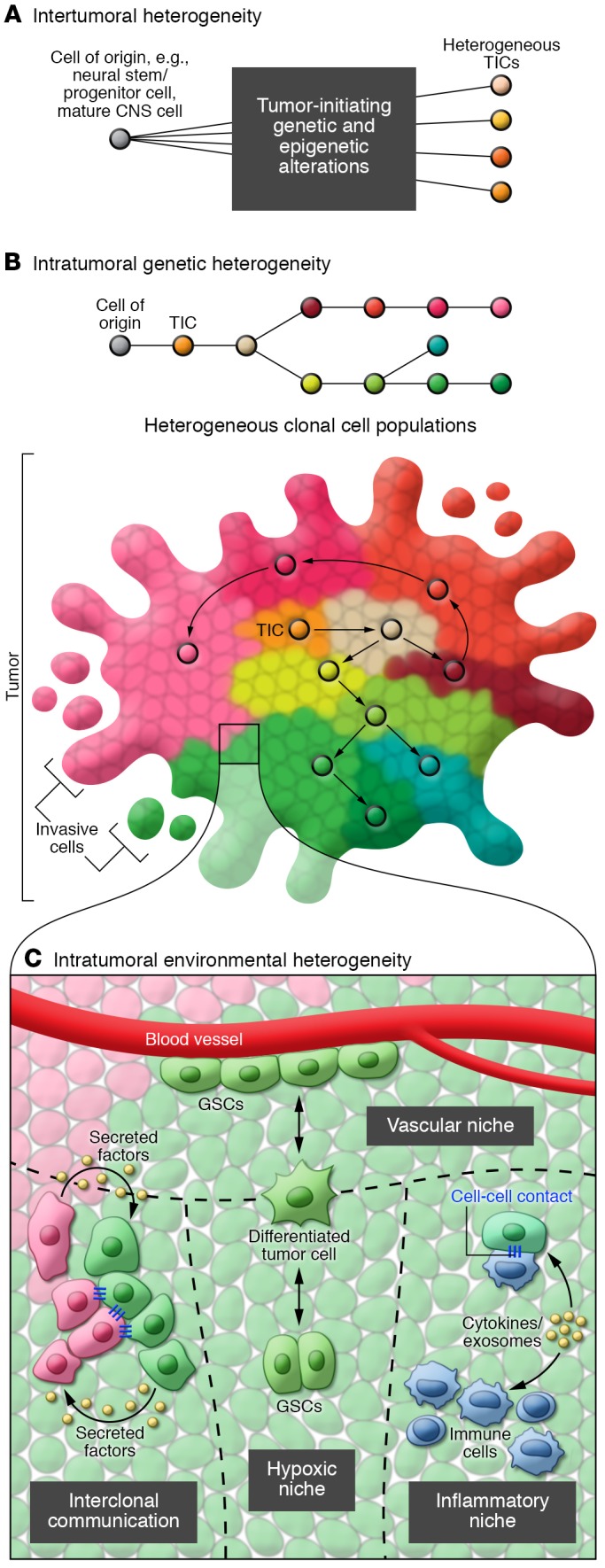
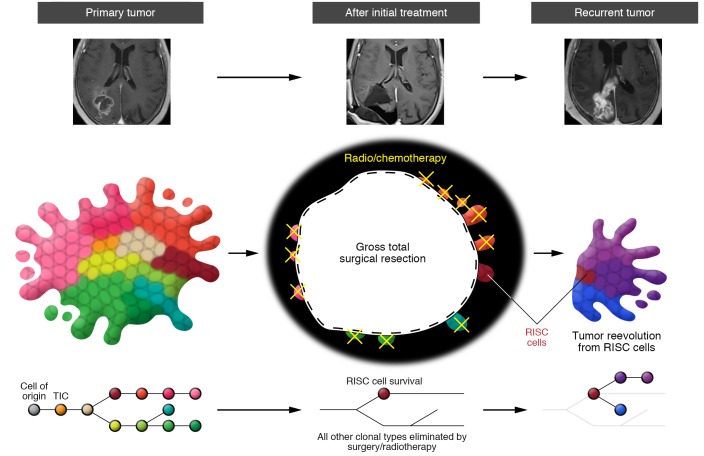
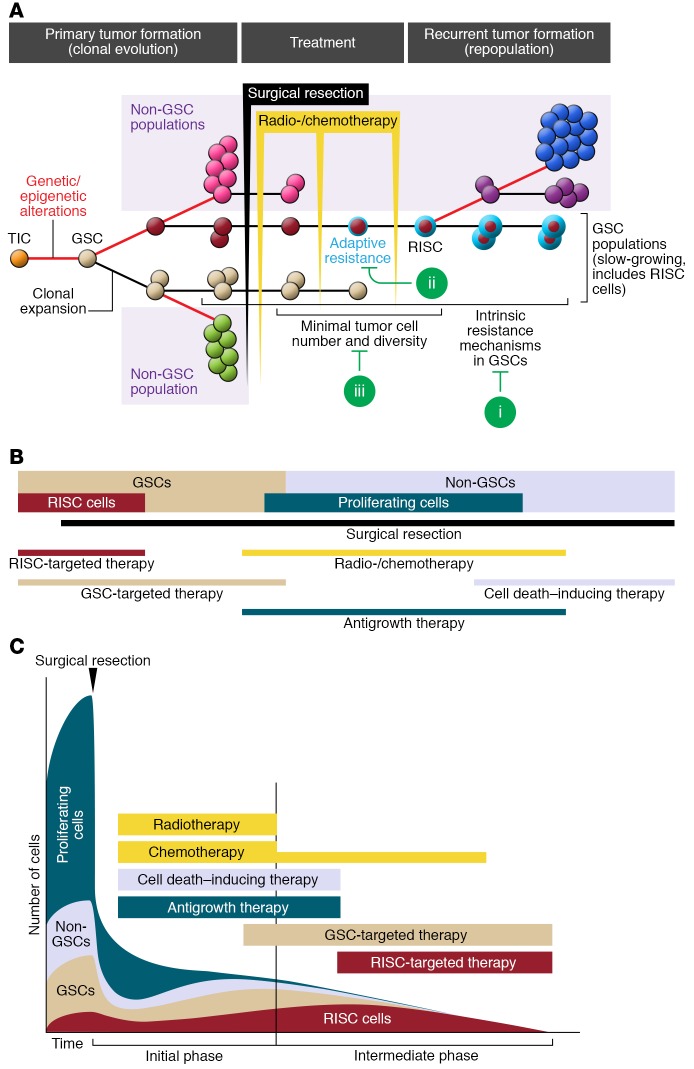
Glioblastoma is the most common and lethal primary malignant brain tumor in adults. Patients die from recurrent tumors that have become resistant to therapy. New strategies are needed to design future therapies that target resistant cells. Recent genomic studies have unveiled the complexity of tumor heterogeneity in glioblastoma and provide new insights into the genomic landscape of tumor cells that survive and initiate tumor recurrence. Resistant cells also co-opt developmental pathways and display stem-like properties; hence we propose to name them recurrence-initiating stem-like cancer (RISC) cells. Genetic alterations and genomic reprogramming underlie the innate and adaptive resistance of RISC cells, and both need to be targeted to prevent glioblastoma recurrence.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
References
-
- Ryken TC, Kalkanis SN, Buatti JM, Olson JJ, AANS/CNS Joint Guidelines Committee The role of cytoreductive surgery in the management of progressive glioblastoma : a systematic review and evidence-based clinical practice guideline. J Neurooncol. 2014;118(3):479–488. doi: 10.1007/s11060-013-1336-7. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
