

Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation
- PMID: 28146296
- PMCID: PMC6464652
- DOI: 10.1002/14651858.CD003212.pub3
Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation
Update in
-
Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation.Cochrane Database Syst Rev. 2023 Jul 27;7(7):CD003212. doi: 10.1002/14651858.CD003212.pub4. Cochrane Database Syst Rev. 2023. PMID: 37497794 Free PMC article. Review.
Abstract
Background: Previous randomised trials and meta-analyses have shown that nasal continuous positive airway pressure (NCPAP) is a useful method for providing respiratory support after extubation. However, this treatment sometimes 'fails' in infants, and they may require endotracheal re-intubation with its attendant risks and expense. Nasal intermittent positive pressure ventilation (NIPPV) can augment NCPAP by delivering ventilator breaths via nasal prongs. Older children and adults with chronic respiratory failure benefit from NIPPV, and the technique has been applied to neonates. However, serious side effects including gastric perforation have been reported with older methods of providing NIPPV.
Objectives: Primary objective To compare effects of management with NIPPV versus NCPAP on the need for additional ventilatory support in preterm infants whose endotracheal tube was removed after a period of intermittent positive pressure ventilation. Secondary objectives To compare rates of gastric distension, gastrointestinal perforation, necrotising enterocolitis and chronic lung disease; duration of hospitalisation; and rates of apnoea, air leak and mortality for NIPPV and NCPAP.
Search methods: We used the standard search strategy of the Cochrane Neonatal Review Group to search the Cochrane Central Register of Controlled Trials (CENTRAL; 2015, Issue 9), MEDLINE via PubMed (1966 to 28 September 2015), Embase (1980 to 28 September 2015) and the Cumulative Index to Nursing and Allied Health Literature (CINAHL; 1982 to 28 September 2015). We also searched clinical trials databases, conference proceedings and reference lists of retrieved articles for randomised controlled trials and quasi-randomised trials.
Selection criteria: We included randomised and quasi-randomised trials comparing use of NIPPV versus NCPAP in extubated preterm infants. NIPPV included non-invasive support delivered by a mechanical ventilator or a bilevel device in a synchronised or non-synchronised way. Participants included ventilated preterm infants who were ready to be extubated to non-invasive respiratory support. Interventions compared were NIPPV, delivered by short nasal prongs or nasopharyngeal tube, and NCPAP, delivered by the same methods.Types of outcomes measures included failure of therapy (respiratory failure, rates of endotracheal re-intubation); gastrointestinal complications (i.e. abdominal distension requiring cessation of feeds, gastrointestinal perforation or necrotising enterocolitis); pulmonary air leak; chronic lung disease (oxygen requirement at 36 weeks' postmenstrual age) and mortality.
Data collection and analysis: Three review authors independently extracted data regarding clinical outcomes including extubation failure; endotracheal re-intubation; rates of apnoea, gastrointestinal perforation, feeding intolerance, necrotising enterocolitis, chronic lung disease and air leak; and duration of hospital stay. We analysed trials using risk ratio (RR), risk difference (RD) and the number needed to treat for an additional beneficial outcome (NNTB) or an additional harmful outcome (NNTH) for dichotomous outcomes, and mean difference (MD) for continuous outcomes. We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to assess the quality of evidence.
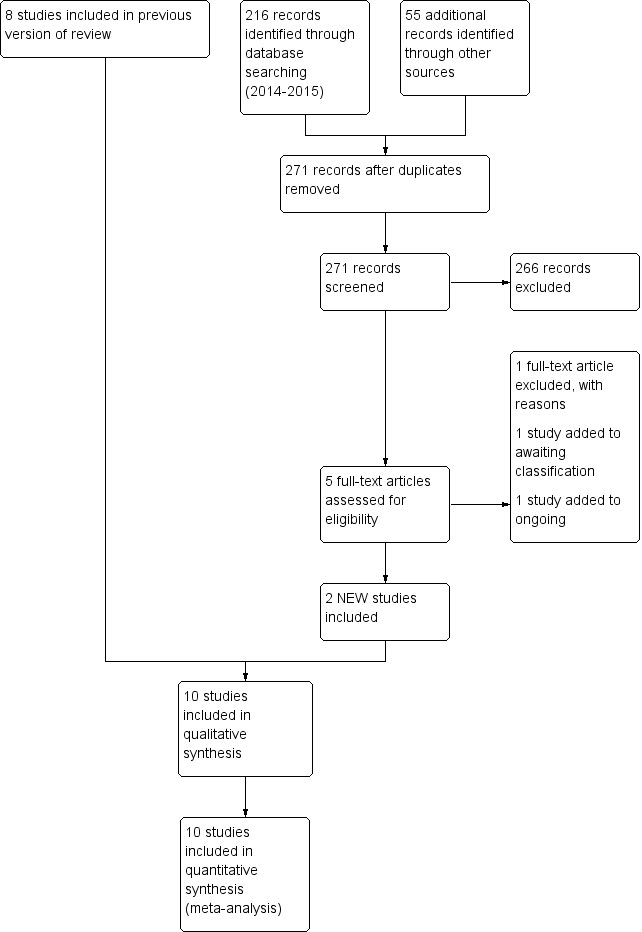
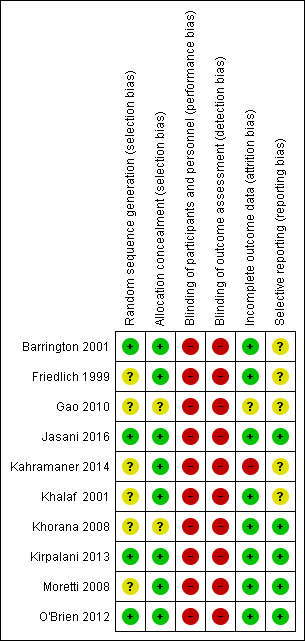
Main results: Through the search, we identified 10 trials enrolling a total of 1431 infants and comparing extubation of infants to NIPPV or NCPAP. Three trials had methodological limitations and possible selection bias.Five trials used the synchronised form of NIPPV, four used the non-synchronised form and one used both methods. Eight studies used NIPPV delivered by a ventilator, one used a bilevel device and one used both methods. When all studies were included, meta-analysis demonstrated a statistically and clinically significant reduction in the risk of meeting extubation failure criteria (typical RR 0.70, 95% CI 0.60 to 0.80; typical RD -0.13, 95% CI -0.17 to -0.08; NNTB 8, 95% CI 6 to 13; 10 trials, 1431 infants) and needing re-intubation (typical RR 0.76, 95% CI 0.65 to 0.88; typical RD -0.10, 95% CI -0.15 to -0.05; NNTB 10, 95% CI 7 to 20; 10 trials, 1431 infants). We graded evidence for these outcomes as moderate, as all trial interventions were unblinded. Although methods of synchronisation varied (Graseby capsule or pneumotachograph/flow-trigger), the five trials that synchronised NIPPV showed a statistically significant benefit for infants extubated to NIPPV in terms of prevention of extubation failure up to one week after extubation.Unsynchronised NIPPV also reduced extubation failure. NIPPV provided via a ventilator is more beneficial than that provided by bilevel devices in reducing extubation failure during the first week. When comparing interventions, investigators found no significant reduction in rates of chronic lung disease (typical RR 0.94, 95% CI 0.80 to 1.10; typical RD -0.02, 95% CI -0.08 to 0.03) or death, and no difference in the incidence of necrotising enterocolitis. Air leaks were reduced in infants randomised to NIPPV (typical RR 0.48, 95% CI 0.28 to 0.82; typical RD -0.03, 95% CI -0.05 to -0.01; NNTB 33, 95% CI 20 to 100). We graded evidence quality as moderate (unblinded studies) or low (imprecision) for secondary outcomes.
Authors' conclusions: Implications for practice NIPPV reduces the incidence of extubation failure and the need for re-intubation within 48 hours to one week more effectively than NCPAP; however, it has no effect on chronic lung disease nor on mortality. Synchronisation may be important in delivering effective NIPPV. The device used to deliver NIPPV may be important; however, data are insufficient to support strong conclusions. NIPPV does not appear to be associated with increased gastrointestinal side effects. Implications for research Large trials should establish the impact of synchronisation of NIPPV on safety and efficacy of the technique and should compare the efficacy of bilevel devices versus a ventilator for providing NIPPV.
Conflict of interest statement
Review authors have declared no conflicts of interest.
Figures
Update of
-
Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation.Cochrane Database Syst Rev. 2014 Sep 4;(9):CD003212. doi: 10.1002/14651858.CD003212.pub2. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2017 Feb 01;2:CD003212. doi: 10.1002/14651858.CD003212.pub3. PMID: 25188554 Updated.
References
References to studies included in this review
Barrington 2001 {published and unpublished data}
-
- Barrington KJ, Finer NN, Bull D. Randomised controlled trial of nasal synchronized intermittent mandatory ventilation compared with continuous positive airway pressure after extubation of very low birth weight infants. Pediatrics 2001;107(4):638‐41. - PubMed
Friedlich 1999 {published data only}
-
- Friedlich P, Lecart C, Posen R, Ramicone E, Chan L, Ramanathan R. A randomized trial of nasopharyngeal‐synchronised intermittent mandatory ventilation versus nasopharyngeal continuous positive airway pressure in very low birth weight infants following extubation. Journal of Perinatology 1999;19(6 Pt 1):413‐8. - PubMed
Gao 2010 {published data only}
-
- Gao WW, Tan SZ, Chen YB, Zhang Y, Wang Y. Randomized trial of nasal synchronized intermittent mandatory ventilation compared with nasal continuous positive airway pressure in preterm infants with respiratory distress syndrome. Chinese Journal of Contemporary Pediatrics 2010;12(7):524‐6. - PubMed
Jasani 2016 {published data only}
-
- Jasani B, Nanavati R, Kabra N, Rajdeo S, Bhandari V. Comparison of non‐synchronized nasal intermittent positive pressure ventilation versus nasal continuous positive airway pressure as post‐extubation respiratory support in preterm infants with respiratory distress syndrome: a randomized controlled trial. Journal of Maternal‐Fetal & Neonatal Medicine 2016;29(10):1546‐51. [PUBMED: 26135774] - PubMed
Kahramaner 2014 {published data only}
-
- Kahramaner Z, Erdemir A, Turkoglu E, Cosar H, Sutcuoglu S, Ozer EA. Unsynchronized nasal intermittent positive pressure versus nasal continuous positive airway pressure in preterm infants after extubation. Journal of Maternal‐Fetal & Neonatal Medicine 2014;27(9):926‐9. [DOI: 10.3109/14767058.2013.846316] - DOI - PubMed
Khalaf 2001 {published data only}
-
- Khalaf MN, Brodsky N, Hurley J, Bhandari V. A prospective randomised controlled trial comparing synchronized nasal intermittent positive pressure ventilation (SNIPPV) versus nasal continuous positive airway pressure (NCPAP) as mode of extubation. Pediatric Research 1999;45:204a. - PubMed
-
- Khalaf MN, Brodsky N, Hurley J, Bhandari V. A prospective randomized, controlled trial comparing synchronized nasal intermittent positive pressure ventilation versus nasal continuous positive airway pressure as modes of extubation. Pediatrics 2001;108(1):13‐7. [MEDLINE: ] - PubMed
Khorana 2008 {published data only}
-
- Khorana M, Paradeevisut H, Sangtawesin V, Kanjanapatanakul W, Chotigeat U, Ayutthaya JKN. A randomized trial of non‐synchronized nasopharyngeal intermittent mandatory ventilation (nsNIMV) vs. nasal continuous positive airway pressure (nCPAP) in the prevention of extubation failure in preterm under 1500 grams. Journal of the Medical Association of Thailand 2008;91(3):S136‐42. - PubMed
Kirpalani 2013 {published and unpublished data}
Moretti 2008 {published data only}
-
- Moretti C, Giannini L, Fassi C, Gizzi C, Papoff P, Colarizi P. Nasal flow‐synchronized intermittent positive pressure ventilation to facilitate weaning in very low‐birthweight infants: unmasked randomized controlled trial. Pediatrics International 2008;50:85‐91. - PubMed
O'Brien 2012 {published data only}
References to studies excluded from this review
Ali 2007 {published data only}
-
- Ali N, Claure N, Alegria X, D'Ugard C, Organero R, Bancalari E. Effects of non‐invasive pressure support ventilation (NI‐PSV) on ventilation and respiratory effort in very low birth weight infants. Pediatric Pulmonology 2007;42:704‐10. - PubMed
Bhandari 2007 {published data only}
-
- Bhandari V, Gavino RG, Nedrelow JH, Pallela P, Salvadore A, Ehrenkranz RA, et al. A randomized controlled trial of synchronized nasal intermittent positive pressure ventilation in RDS. Journal of Perinatology 2007;11:697‐703. - PubMed
Bisceglia 2007 {published data only}
-
- Bisceglia M, Belcastro A, Poerio V, Raimondi F, Mesuraca L, Crugliano C, et al. A comparison of nasal intermittent versus continuous positive pressure delivery for the treatment of moderate respiratory syndrome in preterm infants. Minerva Pediatrica 2007;59:91‐5. - PubMed
DeSimone 2010 {published data only}
-
- DeSimone OA, Sommers R, Destin K, Mance M, Matook S, Stonestreet B, et al. Nasal intermittent positive pressure ventilation (NIPPV) does not facilitate earlier extubation in infants less than 28 weeks gestation: a pilot study. Pediatric Academic Society. 2010.
Kishore 2009 {published data only}
-
- Kishore MSS, Dutta S, Kumar P. Early nasal intermittent positive pressure ventilation versus continuous positive airway pressure for respiratory distress syndrome. Acta Paediatrica 2009;98:1412‐5. - PubMed
Kugelman 2007 {published data only}
-
- Kugelman A, Feferkorn I, Riskin A, Chistyakov I, Kaufman B, Bader D. Nasal intermittent mandatory ventilation versus nasal continuous positive airway pressure for respiratory distress syndrome: a randomized controlled prospective study. Journal of Pediatrics 2007;150:521‐6. - PubMed
Kumar 2011 {published data only}
Lin 1998 {published and unpublished data}
-
- Lin CH, Wang ST, Lin YJ, Yeh TF. Efficacy of nasal intermittent positive pressure ventilation in treating apnea of prematurity. Pediatric Pulmonology 1998;26(5):349‐53. - PubMed
Meneses 2011 {published data only}
-
- Meneses J, Bhandari V, Guilherme AJ, Herrmann D. Noninvasive ventilation for respiratory distress syndrome: a randomized controlled trial. Pediatrics 2011;127(2):300‐7. - PubMed
Moretti 1999 {published data only}
-
- Moretti C, Gizzi C, Papoff P, Lampariello S, Capoferri M, Calcagnini G, et al. Comparing the effects of nasal synchronized intermittent positive pressure ventilation (nSIPPV) and nasal continuous positive airway pressure (nCPAP) after extubation in very low birth weight infants. Early Human Development 1999;56:166‐77. - PubMed
Pantalitschka 2009 {published data only}
-
- Pantalitschka T, Sievers J, Urschitz MS, Herberts T, Reher C, Poets CF. Randomised crossover trial of four nasal respiratory support systems for apnoea of prematurity in very low birthweight infants. Archives of Disease in Childhood. Fetal and Neonatal Edition 2009;94(4):F245‐8. - PubMed
Ramanathan 2012 {published data only}
-
- Ramanathan R, Sekar KC, Rasmussen M, Bhatia J, Soll RF. Nasal intermittent positive pressure ventilation after surfactant treatment for respiratory distress syndrome in preterm infants under 30 weeks gestation: a randomized, controlled trial. Journal of Perinatology 2012;32(5):336‐43. - PubMed
Ryan 1989 {published data only}
-
- Ryan CA, Finer NN, Peters KL. Nasal intermittent positive‐pressure ventilation offers no advantages over nasal continuous positive airway pressure in apnea of prematurity. American Journal of Diseases in Childhood 1989;143(10):1196‐8. - PubMed
Shi 2010 {published data only}
-
- Shi Y, Tang S, Zhao J, Hu Z, Li T. Efficiency of nasal intermittent positive pressure ventilation vs nasal continuous positive airway pressure on neonatal respiratory distress syndrome: a prospective, randomized, controlled study. Acta Academiae Medicinae Militaris Tertiae 2010;32(18):1991‐4.
References to studies awaiting assessment
Silveira 2015 {published data only}
-
- Silveira CS, Leonardi KM, Melo AP, Zaia JE, Brunherotti MA. Response of preterm infants to 2 noninvasive ventilatory support systems: nasal CPAP and nasal intermittent positive‐pressure ventilation. Respiratory Care 2015;60(12):1772‐6. [26374907] - PubMed
References to ongoing studies
El‐Farash 2013 {unpublished data only}
-
- Nasal Continuous Airway Pressure (n‐CPAP) vs Nasal Bilevel Positive Airway Pressure (n‐BiPAP) for RDS. Ongoing study January 2013.
Estay 2013 {unpublished data only}
-
- Non‐Invasive Ventilation vs Continuous Positive Airway Pressure After Extubation in Very Low Birth Weight Infants. Ongoing study December 2011.
NCT02396693 {published data only}
-
- NCT02396693. Successful Extubation and Noninvasive Ventilation in Preterm ≤ 1500g Terms. clinicaltrials.gov/show/NCT02396693 (accessed 7 December 2015).
Shi 2013 {unpublished data only}
-
- Nasal Intermittent Positive Pressure Ventilation in Newborn Infants With Respiratory Distress Syndrome. Ongoing study January 2008.
Victor 2011 {published data only}
-
- Victor S, Extubate Trial Group. EXTUBATE: a randomised controlled trial of nasal biphasic positive airway pressure vs. nasal continuous positive airway pressure following extubation in infants less than 30 weeks' gestation: study protocol for a randomised controlled trial. Trials 2011; Vol. 12:257. - PMC - PubMed
Additional references
Bancalari 2013
-
- Bancalari E, Claure N. The evidence for non‐invasive ventilation in the preterm infant. Archives of Disease in Childhood. Fetal and Neonatal Edition 2013;98(2):F98‐102. - PubMed
Bott 1993
-
- Bott J, Carroll MP, Conway JH, Keilty SE, Ward EM, Brown AM, et al. Randomised controlled trial of nasal ventilation in acute ventilatory failure due to chronic obstructive airways disease. Lancet 1993;341:1555‐7. - PubMed
Davis 2003b
Davis 2009
-
- Davis PG, Morley CJ, Owen LS. Non‐invasive respiratory support of preterm neonates with respiratory distress: continuous positive airway pressure and nasal intermittent positive pressure ventilation. Seminars in Fetal and Neonatal Medicine 2009;14:14‐20. - PubMed
Ellis 1988
-
- Ellis ER, Grunstein RR, Chan S, Bye PT, Sullivan CE. Noninvasive ventilatory support during sleep improves respiratory failure in kyphoscoliosis. Chest 1988;94:811‐5. - PubMed
Garland 1985
-
- Garland JS, Nelson DB, Rice T, Neu J. Increased risk of gastrointestinal perforations in neonates mechanically ventilated with either face mask or nasal prongs. Pediatrics 1985;76:406‐10. - PubMed
GRADEpro 2008 [Computer program]
-
- Brozek J, Oxman A, Schünemann H. GRADEpro. Version 3.2 for Windows. The GRADE Working Group, 2008.
Guyatt 2011a
-
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction ‐ GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. [PUBMED: 21195583] - PubMed
Guyatt 2011b
-
- Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso‐Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence ‐ study limitations (risk of bias). Journal of Clinical Epidemiology 2011;64(4):407‐15. [PUBMED: 21247734] - PubMed
Guyatt 2011c
-
- Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso‐Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence ‐ imprecision. Journal of Clinical Epidemiology 2011;64(12):1283‐93. [PUBMED: 21839614] - PubMed
Guyatt 2011d
-
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 7. Rating the quality of evidence ‐ inconsistency. Journal of Clinical Epidemiology 2011;64(12):1294‐302. [PUBMED: 21803546] - PubMed
Guyatt 2011e
-
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality of evidence ‐ indirectness. Journal of Clinical Epidemiology 2011;64(12):1303‐10. [PUBMED: 21802903] - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. www.cochrane‐handbook.org.
Kiciman 1998
-
- Kiciman NM, Andréasson B, Bernstein G, Mannino FL, Rich W, Henderson C, et al. Thoracoabdominal motion in newborns during ventilation delivered by endotracheal tube or nasal prongs. Pediatric Pulmonology 1998;25:175‐81. - PubMed
Lee 2015
-
- Lee J, Kim HS, Jung YH, Shin SH, Choi CW, Kim EK, et al. Non‐invasive neurally adjusted ventilatory assist in preterm infants: a randomised phase II crossover trial. Archives of Disease in Childhood. Fetal and Neonatal Edition 2015;100(6):F507‐13. - PubMed
Owen 2007
Owen 2008
-
- Owen LS, Morley CJ, Davis PG. Neonatal nasal intermittent positive pressure ventilation: a survey of practice in England. Archives of Disease in Childhood. Fetal and Neonatal Edition 2008;93(2):F148‐50. - PubMed
Owen 2016
-
- Owen LS, Manley BJ. Nasal intermittent positive pressure ventilation in preterm infants: equipment, evidence and synchronization. Seminars in Fetal and Neonatal Medicine 2016;21(3):146‐153. - PubMed
Piper 1992
-
- Piper AJ, Parker S, Torzillo PJ, Sullivan CE, Bye PT. Nocturnal nasal IPPV stabilizes patients with cystic fibrosis and hypercapnic respiratory failure. Chest 1992;102:846‐50. - PubMed
Schünemann 2013
-
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GWG. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. www.guidelinedevelopment.org/handbook. Updated October 2013.
Stein 2012
-
- Stein D, Howard D. Neurally adjusted ventilatory assist in neonates weighing <1500 grams: a retrospective analysis. Journal of Pediatrics 2012;160(5):786‐9. - PubMed
References to other published versions of this review
Davis 2001
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous