

The PHES battery does not detect all cirrhotic patients with early neurological deficits, which are different in different patients
- PMID: 28146589
- PMCID: PMC5287470
- DOI: 10.1371/journal.pone.0171211
The PHES battery does not detect all cirrhotic patients with early neurological deficits, which are different in different patients
Abstract
Background and aims: The psychometric hepatic encephalopathy score (PHES) is the "gold standard" for minimal hepatic encephalopathy (MHE) diagnosis. Some reports suggest that some cirrhotic patients "without" MHE according to PHES show neurological deficits and other reports that neurological alterations are not homogeneous in all cirrhotic patients. This work aimed to assess whether: 1) a relevant proportion of cirrhotic patients show neurological deficits not detected by PHES; 2) cirrhotic patients with mild neurological deficits are a homogeneous population or may be classified in sub-groups according to specific deficits.
Methods: Cirrhotic patients "without" (n = 56) or "with" MHE (n = 41) according to PHES and controls (n = 52) performed psychometric tests assessing attention, concentration, mental processing speed, working memory and bimanual and visuomotor coordination. Heterogeneity of neurological alterations was analysed using Hierarchical Clustering Analysis.
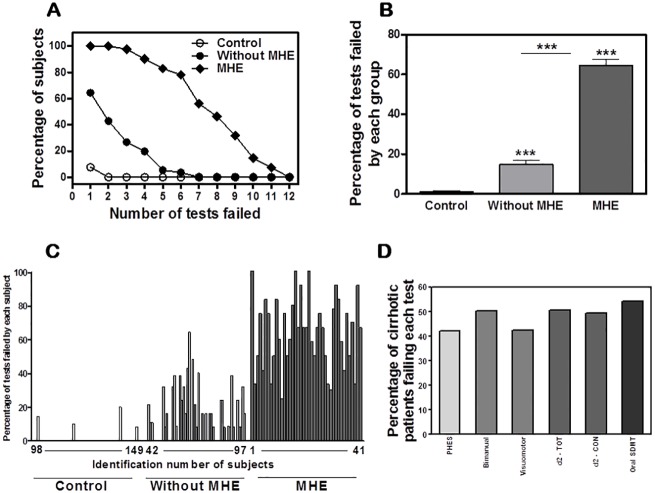
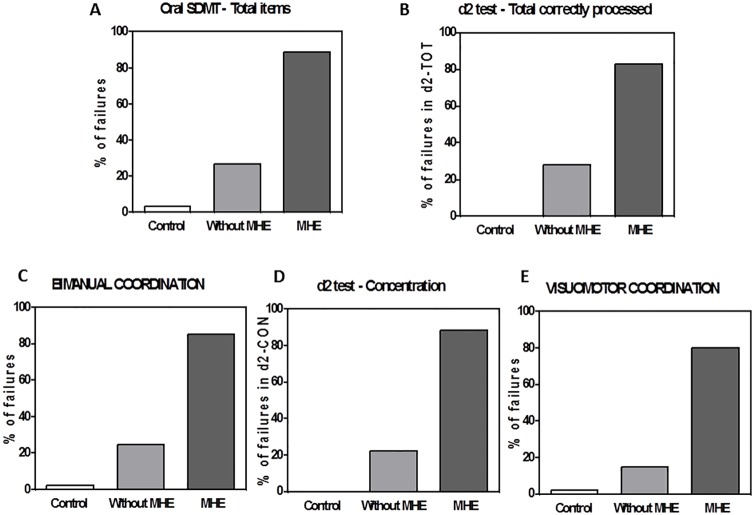
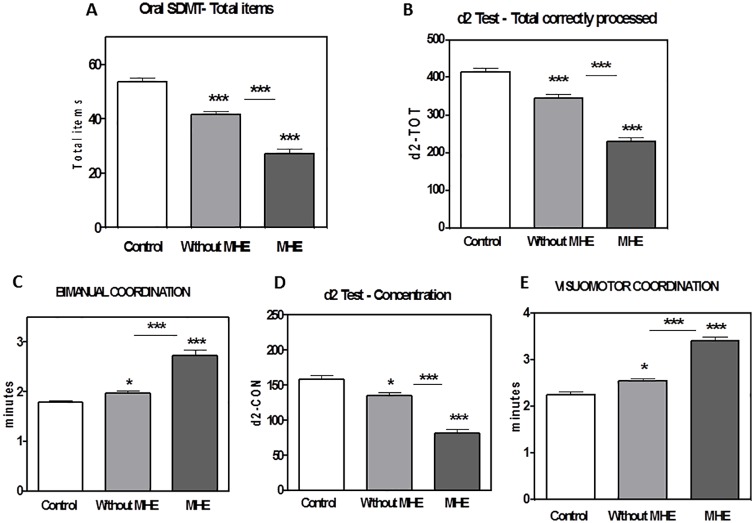
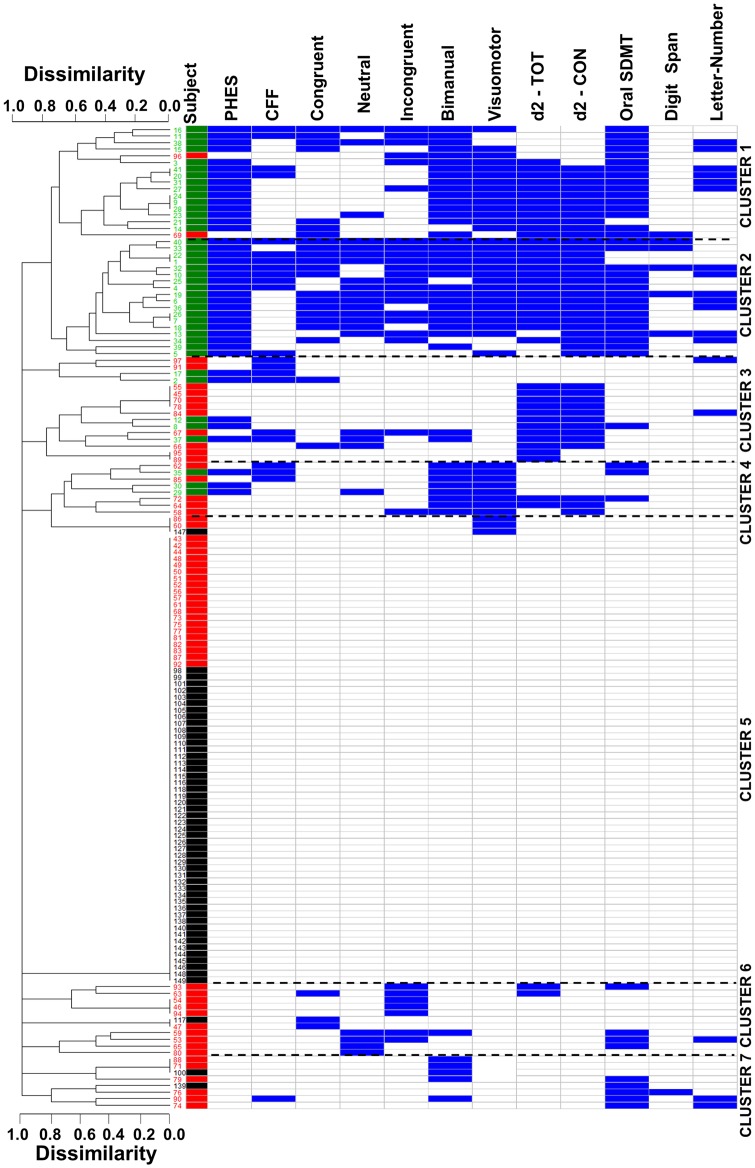
Results: PHES classified as "with" MHE 42% of patients. Around 40% of patients "without" MHE according to PHES fail two psychometric tests. Oral SDMT, d2, bimanual and visuo-motor coordination tests are failed by 54, 51, 51 and 43% of patients, respectively. The earliest neurological alterations are different for different patients. Hierarchical clustering analysis shows that patients "without" MHE according to PHES may be classified in clusters according to the tests failed. In some patients coordination impairment appear before cognitive impairment while in others concentration and attention deficits appear before.
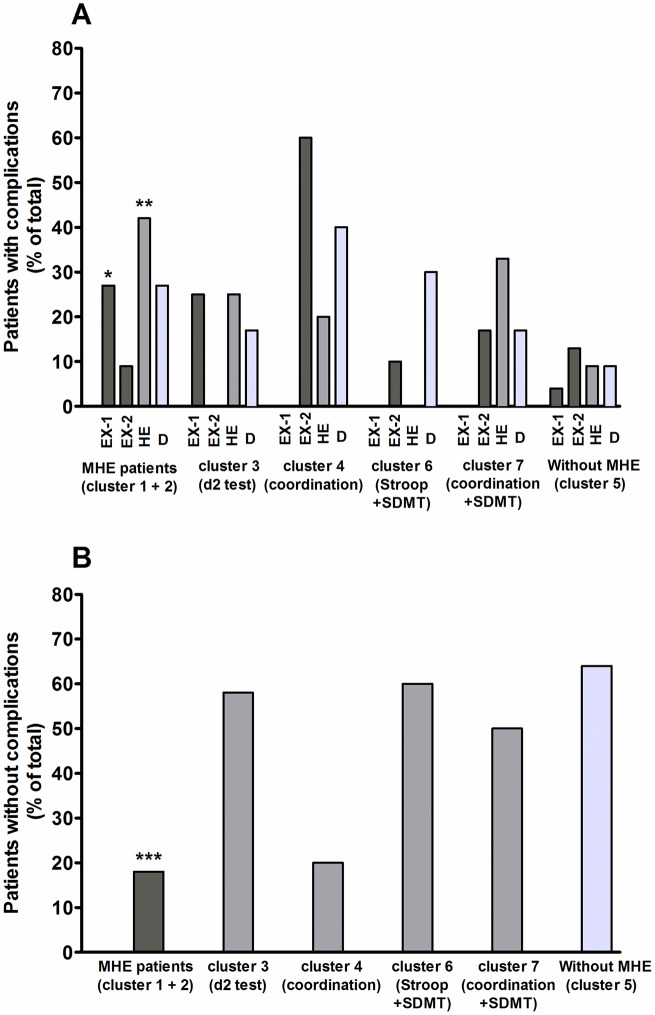
Conclusions: PHES is not sensitive enough to detect early neurological alterations in a relevant proportion of cirrhotic patients. Oral SDMT, d2 and bimanual and visuo-motor coordination tests are more sensitive. The earliest neurological alterations are different in different cirrhotic patients. These data also have relevant clinical implications. Patients classified as "without MHE" by PHES belonging to clusters 3 and 4 in our study have a high risk of suffering clinical complications, including overt HE and must be diagnosed and clinically followed.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT. Hepatic encephalopathy. Definition, nomenclature, diagnosis and quantification: final report of the working party at the 11th World Congress of Gastroenterology, Vienna, 1998. Hepatology. 2002;35:716–721. 10.1053/jhep.2002.31250 - DOI - PubMed
-
- Amodio P, Montagnese S, Gatta A, Morgan MY. Characteristics of minimal hepatic encephalopathy. Metab Brain Dis. 2004;19:253–267. - PubMed
-
- Montoliu C, Piedrafita B, Serra MA, del Olmo JA, Ferrandez A, Rodrigo JM, et al. Activation of soluble guanylate cyclase by nitric oxide in lymphocytes correlates with minimal hepatic encephalopathy in cirrhotic patients. J Mol Med. 2007;85:233–241. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
