

"It's about my life": facilitators of and barriers to isoniazid preventive therapy completion among people living with HIV in rural South Africa
- PMID: 28147705
- PMCID: PMC5545149
- DOI: 10.1080/09540121.2017.1283390
"It's about my life": facilitators of and barriers to isoniazid preventive therapy completion among people living with HIV in rural South Africa
Abstract
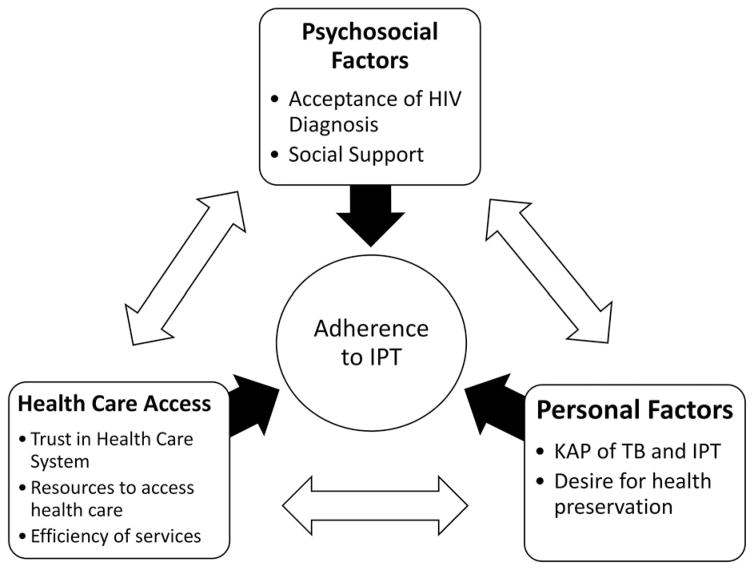
Despite the recent rollout of Isoniazid Preventive Therapy (IPT) to prevent TB in people living with HIV in South Africa, adherence and completion rates are low. To explore barriers to IPT completion in rural KwaZulu-Natal, South Africa, we conducted individual semi-structured interviews among 30 HIV patients who had completed or defaulted IPT. Interview transcripts were analyzed according to the framework method of qualitative analysis. Facilitators of IPT completion included knowledge of TB and IPT, accepting one's HIV diagnosis, viewing IPT as similar to antiretroviral therapy, having social support in the community and the clinic, trust in the healthcare system, and desire for health preservation. Barriers included misunderstanding of IPT's preventive role in the absence of symptoms, inefficient health service delivery, ineffective communication with healthcare workers, financial burden of transport to clinic and lost wages, and competing priorities. HIV-related stigma was not identified as a significant barrier to IPT completion, and participants felt confident in their ability to manage stigma, for example by pretending their medications were for unrelated conditions. Completers were more comfortable communicating with health care workers than were defaulters. Efforts to facilitate successful IPT completion must include appropriate counseling and education for individual patients and addressing inefficiencies within the health care system in order to minimize patients' financial and logistical burden. These patient-level and structural changes are necessary for IPT to successfully reduce TB incidence in this resource-limited setting.
Keywords: HIV/AIDS; Isoniazid preventive therapy; adherence; qualitative methods; tuberculosis.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical