

Severity-dependent differences in early management of thoracic trauma in severely injured patients - Analysis based on the TraumaRegister DGU®
- PMID: 28148274
- PMCID: PMC5288852
- DOI: 10.1186/s13049-017-0354-4
Severity-dependent differences in early management of thoracic trauma in severely injured patients - Analysis based on the TraumaRegister DGU®
Abstract
Background: Major trauma is associated with chest injuries in nearly 50% of multiple injuries. Thoracic trauma is a relevant source of comorbidity throughout the period of multiply-injured patient care and may require swift and well-thought-out interventions in order to avert a deleterious outcome. In this epidemiological study we seek to characterize groups of different thoracic trauma severity in severely injured patients and identify related differences in prehospital and early clinical management. This may help to anticipate necessary treatment for chest injuries.
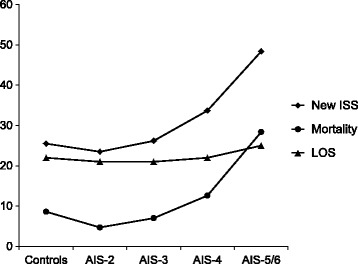
Methods: Patients documented between 2002 and 2012 in the TraumaRegister DGU®, aged ≥ 16 years, determined Injury Severity Score ≥ 16, and documentation from European trauma centers were analyzed. Isolated brain injury and severe head injury (Abbreviated Injury ScaleHead ≥ 4) led to patient exclusion. Patient subgroups were formed according to the Abbreviated Injury ScaleThorax as Controls, AIS-2, AIS-3, AIS-4, and AIS-5/6. Demographic and clinical characteristics comparing the aforementioned groups were evaluated using descriptive statistics.
Results: Twenty two thousand five hundred sixty five predominantly male (74%) patients, mean age 45.7 years (SD 19.3), suffering from blunt trauma (95%), and presenting a mean Injury Severity Score of 25.6 (SD 9.6) were analyzed. Higher thoracic injury severity was associated with more different thoracic injuries. The highest rate of prehospital intubation (58%) occurred in AISThorax-5/6. The worse the chest trauma, the more chest tubes were placed prehospitally, peaking at 22% in AISThorax-5/6. Out-of-hospital cardiopulmonary resuscitation was successfully performed in 11% in AISThorax-5/6 compared to 1%-3% in lesser thoracic trauma severity. Massive transfusion and emergency surgery was highest in AISThorax-5/6 compared to lesser thoracic injury (12% vs. 5%-7% and 17% vs. 3%-7%) and both were independently associated with thoracic injuries in patients with AISThorax ≥ 4.
Conclusions: We provide epidemiological data on trauma mechanism, concomitant injuries, frequencies of emergency interventions and outcome associated with different thoracic trauma severity. Prehospital and early clinical management is more complex when AISThorax is ≥ 4. Severely injured patients with critical thoracic trauma are most challenging to take care of with highest rates in prehospital intubation, cardiopulmonary resuscitation, chest tube placements, blood transfusions as well as emergency surgery.
Keywords: Chest injury; Emergency management; Emergency procedures; Polytrauma; Severely injured; Thoracic trauma.
Figures
References
-
- Vecsei V, Arbes S, Aldrian S, Nau T. Chest injuries in polytrauma. Eur J Trauma. 2005;31:239–43. doi: 10.1007/s00068-005-2033-9. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
