

Tethering the Extensor Apparatus Limits PIP Flexion Following K-wire Placement for Pinning Extra-articular Fractures at the Base of the Proximal Phalanx
- PMID: 28149210
- PMCID: PMC5256656
- DOI: 10.1177/1558944716628498
Tethering the Extensor Apparatus Limits PIP Flexion Following K-wire Placement for Pinning Extra-articular Fractures at the Base of the Proximal Phalanx
Abstract
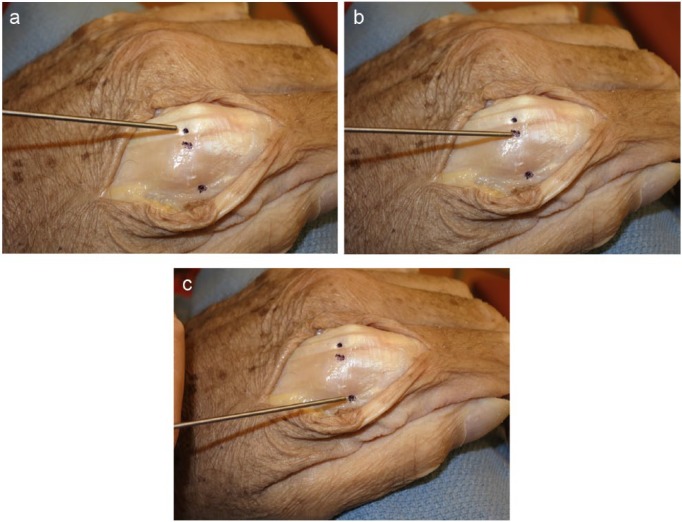
Background: Closed reduction with percutaneous Kirschner wires (K-wires) is the most minimally invasive surgical option for stabilizing phalanx fractures. This study examines the effect of K-wire placement on proximal interphalangeal (PIP) joint motion. Methods: PIP joint flexion was measured in the digits of 4 fresh-frozen cadaver hands after placing a suture loop through the flexor tendons and placing tension on the flexors via a mechanical scale. The load necessary to flex the PIP joint to 90° or to maximum flexion was recorded. The load was removed and K-wires were inserted in 3 locations about the metacarpophalangeal joint (MPJ): through the extensor tendon and across the MPJ, adjacent to the extensor tendon insertion site and across the MPJ, and through the sagittal band and into the base of the proximal phalanx (P1). The load on the tendons was reapplied, and angles of PIP joint flexion were recorded for each of the 3 conditions. Results: The mean angle of PIP joint flexion prior to K-wire insertion was 87°, and the mean load applied was 241 g. The angles of flexion were 53° when the K-wire was placed through the extensor tendon, 70° when the K-wire was placed adjacent to the tendon, and 75° when the K-wire was placed into the base of P1 by going through the sagittal band, midway between the volar plate and the extensor tendon. Conclusions: K-wires placed remote from the extensor tendon create less of an immediate tether to PIP joint flexion than those placed through or adjacent to the extensor tendon.
Keywords: Kirschner wires fixation; extensor tendon; joint stiffness; proximal interphalangeal joint motion; proximal phalanx fracture.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark E. Baratz has received consultant fees and royalties from Integra LifeSciences and consultant fees from Elizur.
Figures

References
-
- Al-Qattan MM. Phalangeal neck fractures of the proximal phalanx of the fingers in adults. Injury. 2010;41(10):1084-1089. - PubMed
-
- Al-Qattan MM, Al-Zaharani K. Open reduction and cerclage wire fixation for long oblique/spiral fractures of the proximal phalanx of the fingers. J Hand Surg Eur. 2008;33(2):170-173. - PubMed
-
- Belsky MR, Eaton RG, Lane LB. Closed reduction and internal fixation of proximal phalangeal fractures. J Hand Surg Am. 1984;9:725-729. - PubMed
-
- Elmaraghy MW, Elmaraghy AW, Richards RS, Chinchalkar SJ, Turner R, Roth JH. Transmetacarpal intramedullary K-wire fixation of proximal phalangeal fractures. Ann Plast Surg. 1998;41:125-130. - PubMed
-
- Faruqui S, Stern PJ, Kiefhaber TR. Percutaneous pinning of fractures in the proximal third of the proximal phalanx: complications and outcomes. J Hand Surg Am. 2012;37:1342-1348. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
