

Management of acute postoperative pain with continuous intercostal nerve block after single port video-assisted thoracoscopic anatomic resection
- PMID: 28149550
- PMCID: PMC5227235
- DOI: 10.21037/jtd.2016.12.30
Management of acute postoperative pain with continuous intercostal nerve block after single port video-assisted thoracoscopic anatomic resection
Abstract
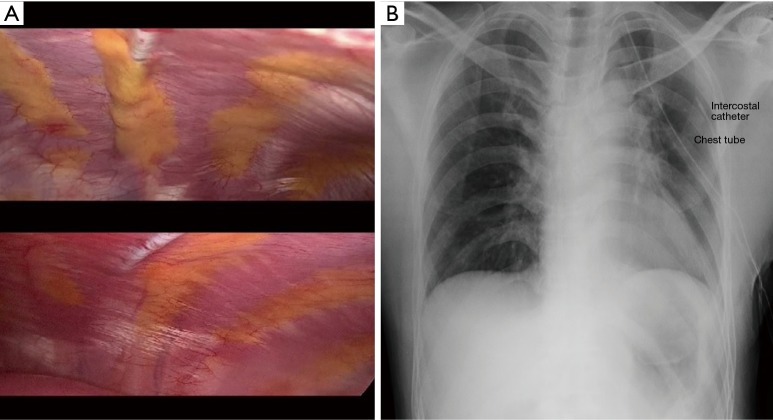
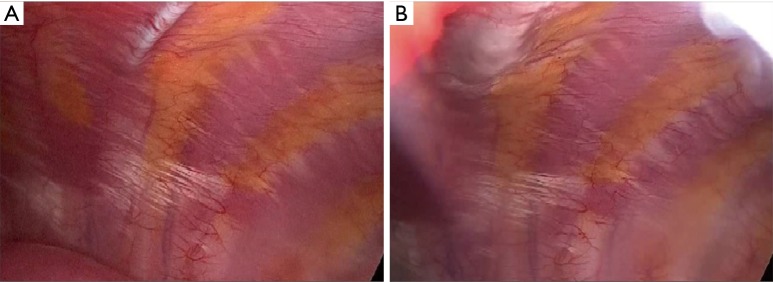
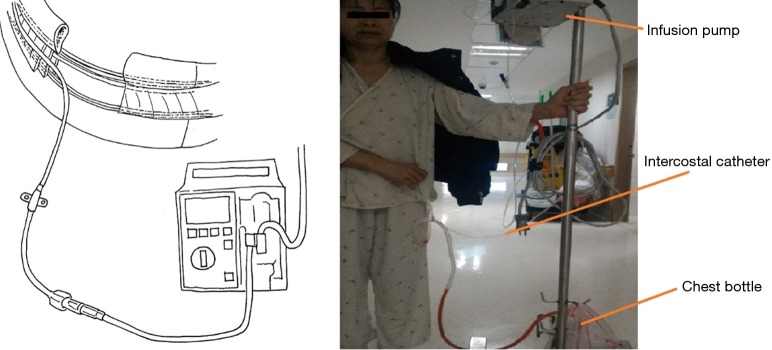
Background: Effective postoperative pain control for thoracic surgery is very important, not only because it reduces pulmonary complications but also because it accelerates the pace of recovery. Moreover, it increases patients' satisfaction with the surgery. In this study, we present a simple approach involving the safe placement of intercostal catheter (ICC) after single port video-assisted thoracoscopic surgery (VATS) anatomic resection and we evaluate postoperative analgesic function with and without it.
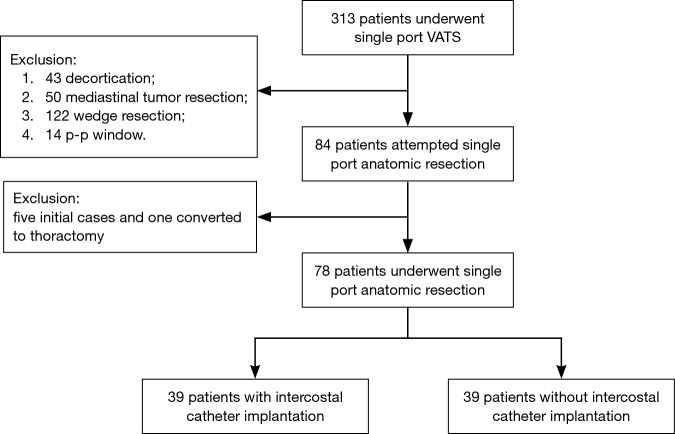
Methods: We identified patients who underwent single port anatomic resection with ICC placed intraoperatively as a route for continuous postoperative levobupivacaine (0.5%) administration and retrospectively compared them with a group of single port anatomic resection patients without ICC. The operation time, postoperative day 0, 1, 2, 3 and discharge day pain score, triflow numbers, narcotic requirements, drainage duration and post-operative hospital stay were compared.
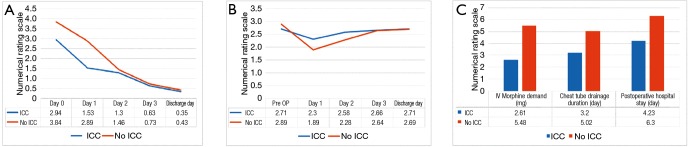
Results: In total, 78 patients were enrolled in the final analysis (39 patients with ICC and 39 without). We found patients with ICC had less pain sensation numerical rating scale (NRS) on postoperative day 0, 1 (P=0.023, <0.001) and better triflow performance on postoperative day 1 and 2 (P=0.015, 0.032). In addition, lower IV form morphine usage frequency and dosage (P=0.009, 0.017), shorter chest tube drainage duration (P=0.001) and postoperative stay (P=0.005) were observed in the ICC group.
Conclusions: Continuous intercostal nerve blockade by placing an ICC intraoperatively provides effective analgesia for patients undergoing single port VATS anatomic resection. This may be considered a viable alternative for postoperative pain management.
Keywords: Single port VATS; anatomic resection; intercostal nerve block.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
-
- American Society of Anesthesiologists Task Force on Acute Pain Management . Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2012;116:248-73. 10.1097/ALN.0b013e31823c1030 - DOI - PubMed
-
- Ghaly G, Kamel M, Nasar A, et al. Video-Assisted Thoracoscopic Surgery Is a Safe and Effective Alternative to Thoracotomy for Anatomical Segmentectomy in Patients With Clinical Stage I Non-Small Cell Lung Cancer. Ann Thorac Surg 2016;101:465-72; discussion 472. 10.1016/j.athoracsur.2015.06.112 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical