

Thoracoscopic esophageal repair with barbed suture material in a case of Boerhaave's syndrome
- PMID: 28149585
- PMCID: PMC5227234
- DOI: 10.21037/jtd.2016.12.46
Thoracoscopic esophageal repair with barbed suture material in a case of Boerhaave's syndrome
Abstract
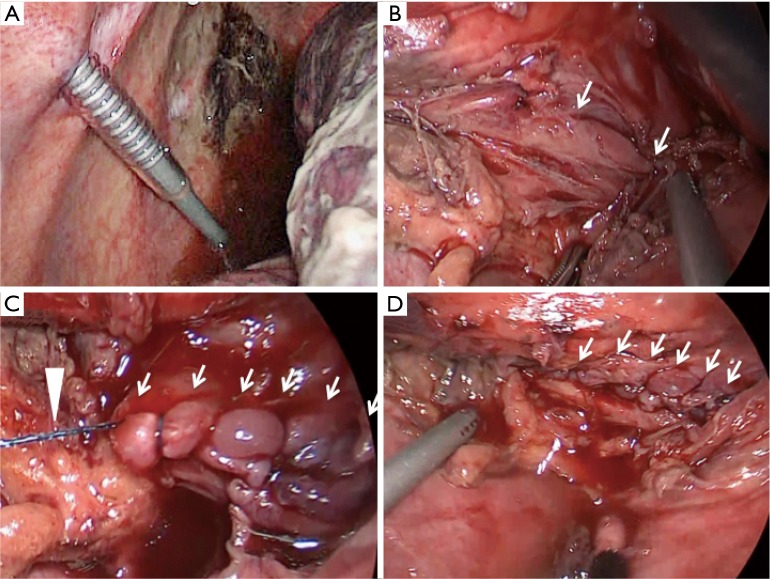
A 53-year-old man was referred to our hospital with Boerhaave's syndrome. Thirty hours after onset, a left thoracoscopic operation was performed, with carbon dioxide pneumothorax and the patient in right semi-prone position. The thoracic cavity was copiously irrigated with physiological saline and a 4-cm longitudinal rupture was identified on the left side of the lower esophagus. The esophageal injury was repaired in 2 layers by using barbed absorbable suture material. The patient was allowed oral feeds after contrast esophagography confirmed the absence of contrast leak at the sutured site on postoperative day 7, and discharged by day 28. Suturing of the ruptured esophagus under thoracoscopic guidance is considered to be difficult and requires expertise. This case report demonstrates that the use of a barbed suture material simplifies thoracoscopic esophageal repair and also highlights the importance of pneumothorax and patient position in improving access to the esophagus.
Keywords: Spontaneous esophageal rupture; barbed absorbable suture; carbon dioxide; pneumothorax.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures



Similar articles
-
Laparoscopic transhiatal suture closure for spontaneous esophageal rupture: a case report.Surg Case Rep. 2019 Oct 22;5(1):149. doi: 10.1186/s40792-019-0711-9. Surg Case Rep. 2019. PMID: 31641962 Free PMC article.
-
Thoracoscopic primary repair with mediastinal drainage is a viable option for patients with Boerhaave's syndrome.J Thorac Dis. 2018 Feb;10(2):784-789. doi: 10.21037/jtd.2018.01.50. J Thorac Dis. 2018. PMID: 29607149 Free PMC article.
-
Septic shock revealing boerhaave's syndrome a case report.Int J Surg Case Rep. 2024 Apr;117:109482. doi: 10.1016/j.ijscr.2024.109482. Epub 2024 Mar 11. Int J Surg Case Rep. 2024. PMID: 38471207 Free PMC article.
-
Minimally invasive surgical management of Boerhaave's syndrome: a narrative literature review.J Thorac Dis. 2020 Aug;12(8):4411-4417. doi: 10.21037/jtd-20-1020. J Thorac Dis. 2020. PMID: 32944354 Free PMC article. Review.
-
Boerhaave's syndrome presenting with abdominal pain and right hydropneumothorax.Am J Emerg Med. 1996 Jan;14(1):53-6. doi: 10.1016/S0735-6757(96)90016-9. Am J Emerg Med. 1996. PMID: 8630158 Review.
Cited by
-
Usefulness of lavage and drainage using video-assisted thoracoscopic surgery for Boerhaave's syndrome: a retrospective analysis.J Thorac Dis. 2021 Jun;13(6):3420-3425. doi: 10.21037/jtd-20-2445. J Thorac Dis. 2021. PMID: 34277038 Free PMC article.
-
Effects of the lavage through fistula in treatment of spontaneous esophageal rupture by combined thoracoscopic and gastroscopic management.World J Emerg Surg. 2025 Jun 7;20(1):51. doi: 10.1186/s13017-025-00630-6. World J Emerg Surg. 2025. PMID: 40483493 Free PMC article.
-
Treatment of spontaneous esophageal rupture (Boerhaave syndrome) using thoracoscopic surgery and sivelestat sodium hydrate.J Thorac Dis. 2018 Apr;10(4):2206-2212. doi: 10.21037/jtd.2018.03.136. J Thorac Dis. 2018. PMID: 29850124 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources