

doi: 10.1016/j.eats.2016.08.024.
eCollection 2016 Dec.
Arthroscopic Superior Capsular Reconstruction for Massive Irreparable Rotator Cuff Repair
Affiliations
- PMID: 28149739
- PMCID: PMC5264010
- DOI: 10.1016/j.eats.2016.08.024
Item in Clipboard
Arthroscopic Superior Capsular Reconstruction for Massive Irreparable Rotator Cuff Repair
Arthrosc Tech.
.
Abstract
We have been performing arthroscopic superior capsular reconstruction (SCR) with acellular dermal allograft for almost 2 years. Our techniques are based on Mihata's original concept for SCR, in which he used fascia lata autograft. In this report, we describe our standard arthroscopic technique as well as 2 variations of a "zip-line" technique, which we have found particularly useful for large dermal allografts (grafts that are ≥40 mm in any dimension).
Figures
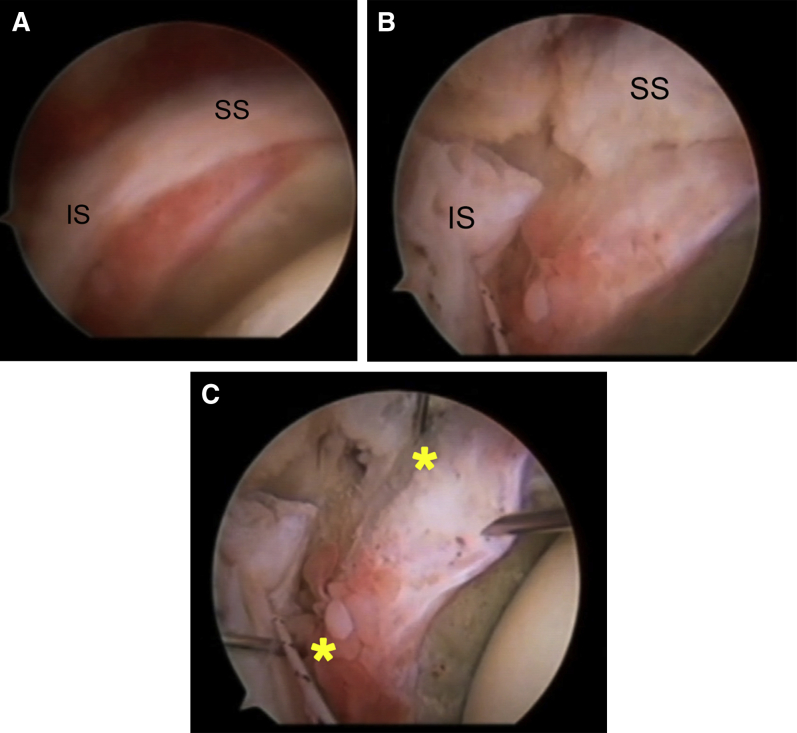
(A) Right shoulder, posterolateral viewing portal. Supraspinatus (SS) and infraspinatus (IS) obscure visualization of superior glenoid neck and impedes bone bed preparation. (B) Right shoulder, posterolateral viewing portal. After posterior interval slide, there is increased working space between the SS and IS to allow bone bed preparation to be performed more easily. (C) Right shoulder, posterolateral viewing portal. Anterior and posterior anchors (*) have been placed in the superior glenoid neck after performing posterior interval slide. Note that the exposure is much better than in (A), before the posterior interval slide was performed. Placement of anterior and posterior anchors into superior glenoid neck has been expedited by the expanded exposure afforded by posterior interval slide.
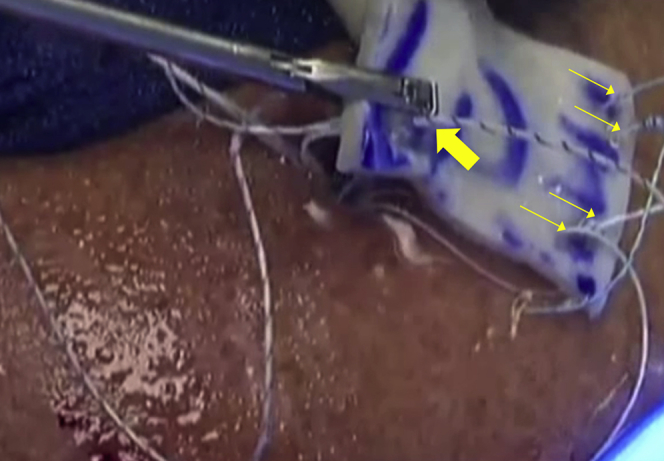
Right shoulder, exterior view. Dermal allograft lying on top of lateral portal, just before passage into joint. Small arrows show sutures from glenoid anchors after mulberry knots have been tied; heavy arrow shows one FiberTape from medial row humeral anchors as another FiberTape is being passed.
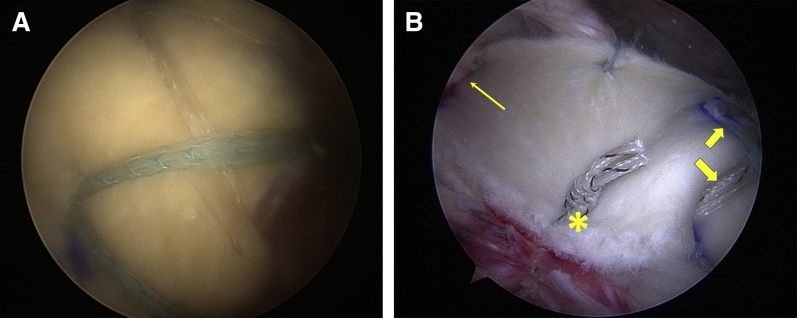
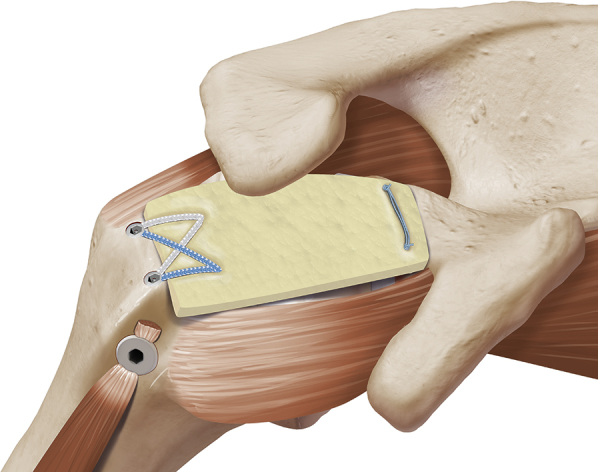
(A) Right shoulder, posterolateral viewing portal. Suture tapes from medial row of humeral fixation have been tensioned and have been secured by a lateral row of suture anchors. (B) Final construct of superior capsular reconstruction showing medial sutures (thin arrow); lateral fixation with FiberTapes (heavy arrows); and side-to-side fixation of dermal graft to infraspinatus (asterisk).
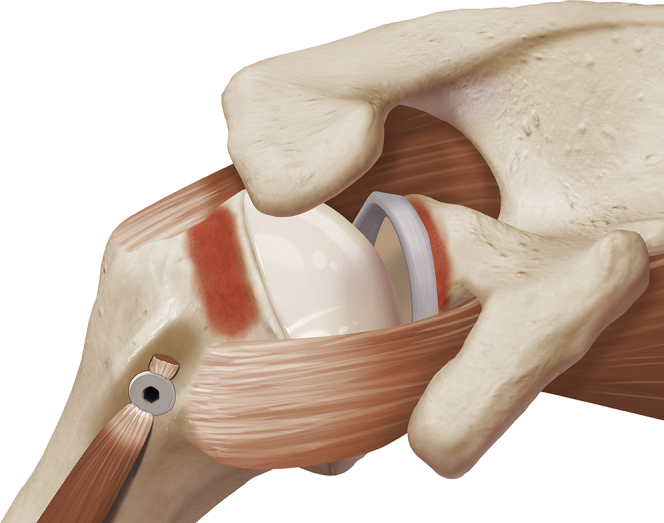
Residual defect in a right shoulder after repairing as much of the rotator cuff as possible.
Right shoulder. Bone bed preparation on the superior glenoid and the greater tuberosity has been performed with a combination of ring curettes, motorized shavers, and motorized burrs.
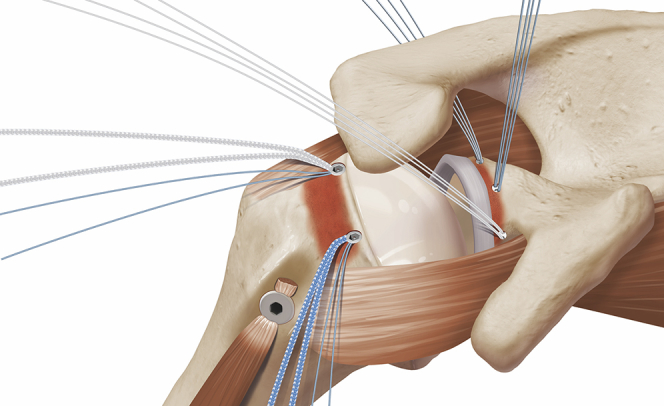
Right shoulder. Three glenoid suture anchors (BioComposite SutureTaks; Arthrex) are placed. In addition, 2 BioComposite SwiveLock-C suture anchors (Arthrex) are placed into the greater tuberosity at the articular margin of the proximal humerus.
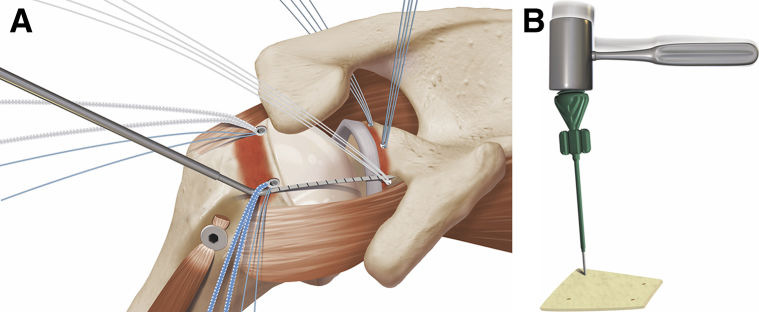
Right shoulder. (A) A flexible calibrated probe (Arthrex) is used to size the graft by measuring the distance between all 5 suture anchors. (B) The inserter for a SwiveLock-C suture anchor (Arthrex) is used as a punch to make 4 punch-holes for passage of the sutures from the 4 corners of the anchor construct.
Right shoulder. Medial sutures have been passed through the graft extracorporeally. Cinch-loops have been placed in the 2 lateral punch-holes for later shuttling of the FiberTapes.
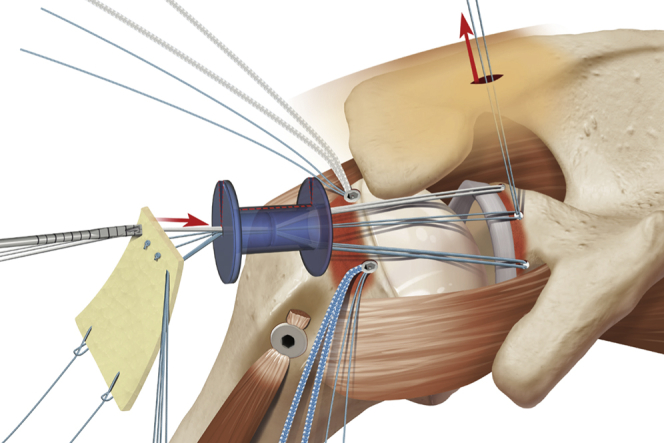
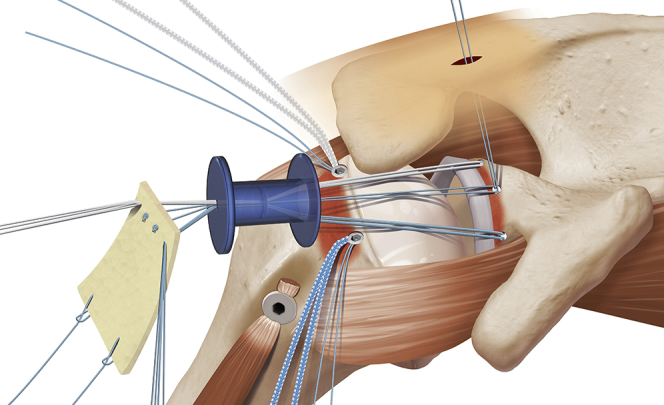
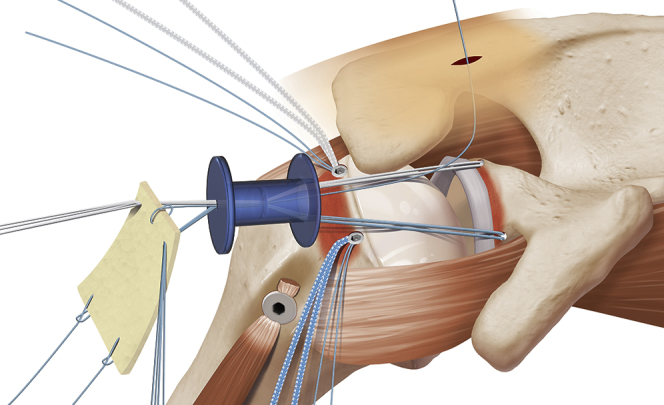
Right shoulder. The PassPort cannula has been split (dotted red line) to allow for expansion or removal of the cannula in order to accommodate the oversized graft. The 2 zip-lines are the anterior and posterior groups of glenoid sutures. A calibrated Zip Line pusher (Arthrex) is used to alternately push the graft down the tensioned anterior and posterior zip-lines. At the same time, the sutures from the middle glenoid anchor are tensioned in order to pull the graft into place over the superior glenoid.
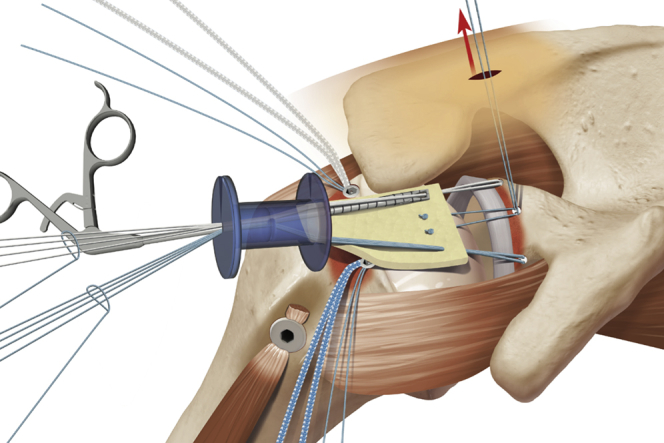
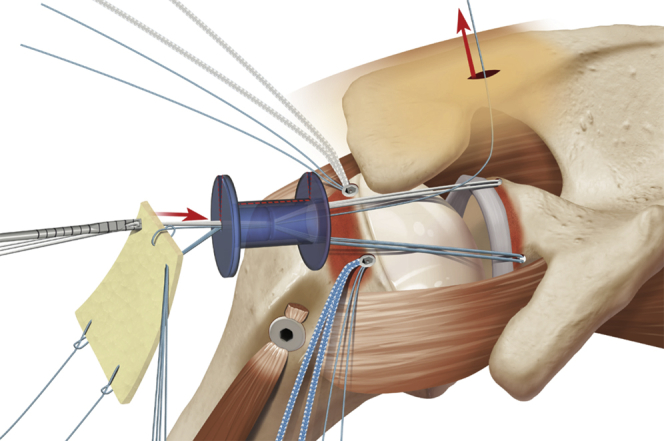
Right shoulder. The calibrated Zip Line pusher (Arthrex) is pushing the graft down the posterior zip-line as the middle glenoid sutures pull the graft into position over the superior glenoid.
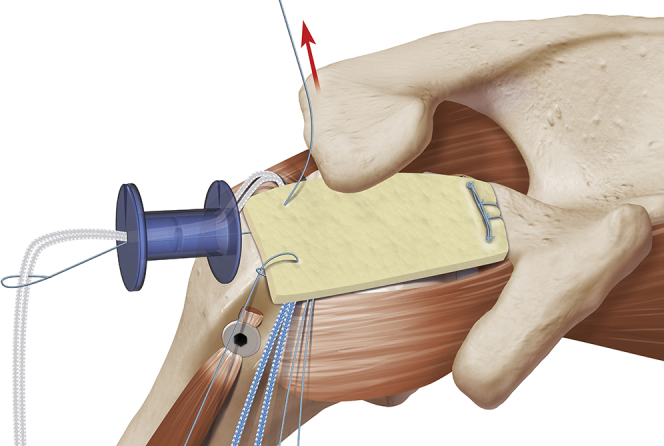
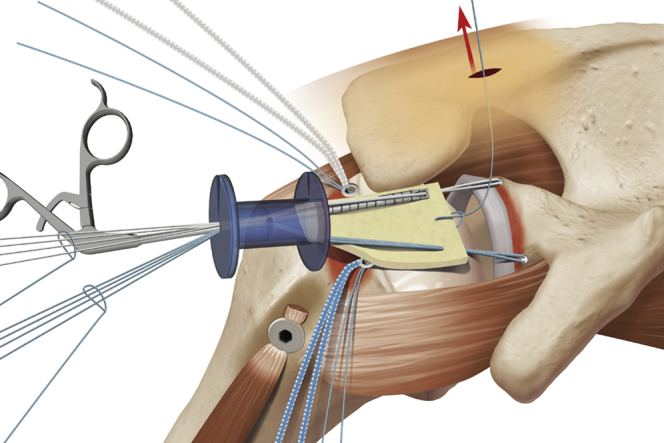
Right shoulder. The lateral cinch-loops (FiberLink; Arthrex) have been “un-cinched,” and are used to shuttle the FiberTapes through the lateral punch-holes in the graft.
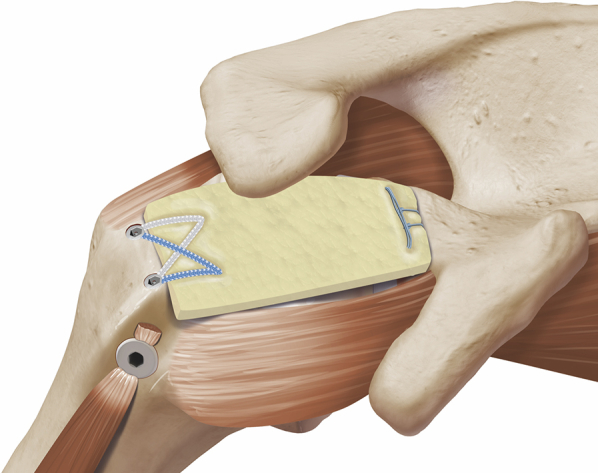
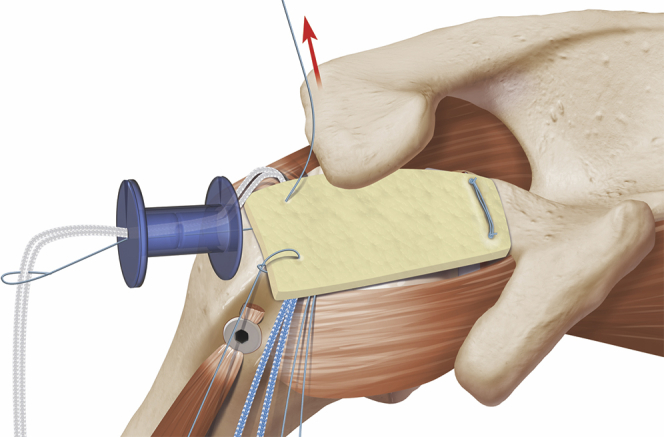
Right shoulder. Lateral fixation of the graft has been achieved by criss-crossing the FiberTapes and securing them with 2 BioComposite SwiveLock-C suture anchors (Arthrex) in a SpeedBridge configuration.
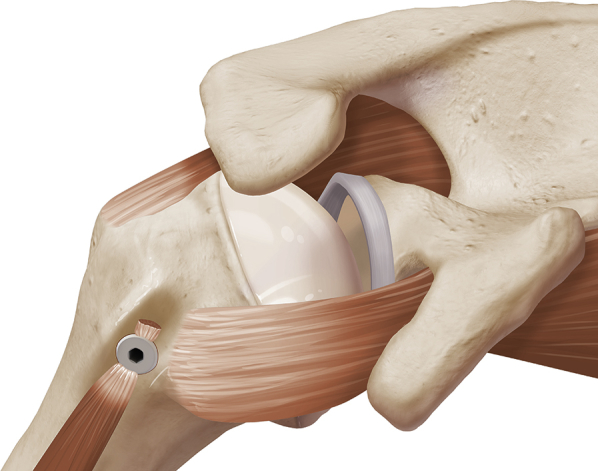
Right shoulder. Residual defect in the rotator cuff after repairing all reparable elements of the rotator cuff tear.
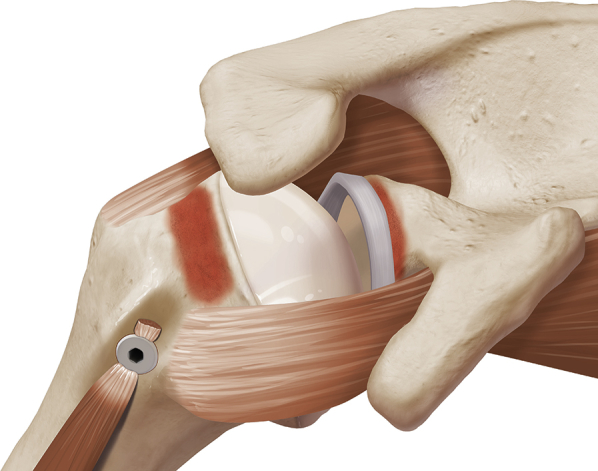
Right shoulder. The bone beds on the superior glenoid and the greater tuberosity have been prepared.
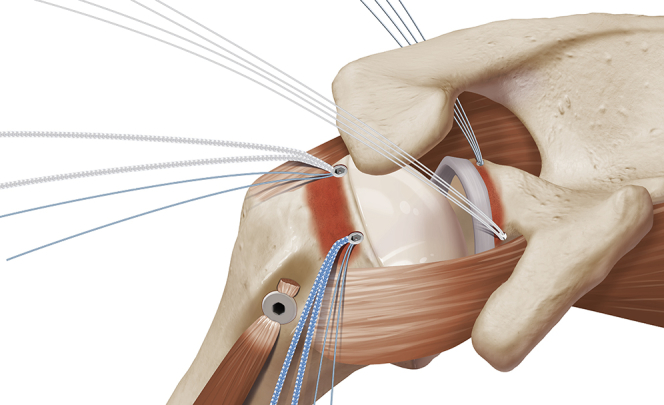
Right shoulder. Two suture anchors (BioComposite SutureTaks; Arthrex) have been placed in the superior glenoid, and 2 additional anchors (BioComposite SwiveLocks preloaded with FiberTape) have been placed at the articular margin of the greater tuberosity of the proximal humerus.
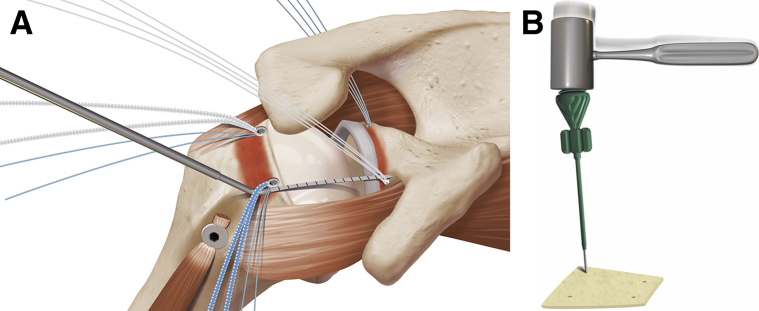
Right shoulder. (A) A flexible calibrated probe is used to size the graft by measuring the distances between all 4 suture anchors. (B) The SwiveLock Inserter (Arthrex) is used as a punch to create 4 holes in the graft corresponding to the locations of the underlying suture anchors.
Right shoulder. Shuttling sutures and graft fixation sutures are passed through the graft extracorporeally. Tapes are not passed through the graft at this stage; they will be shuttled after medial fixation has been completed.
Right shoulder. A calibrated Zip Line pusher (Arthrex) is used to push the graft through the cannula by alternately pushing the graft down the 2 zip-lines as the medial “pulling suture” is tensioned. Note that the PassPort cannula has been split (red dotted line) and may either be expanded or removed to permit graft passage.
Right shoulder. Once the graft is inside the shoulder, the Zip Line pusher (Arthrex) again pushes the graft down the 2 zip-lines as the “pulling suture” is tensioned.
Right shoulder. Medial fixation of the graft to the superior glenoid is achieved by using a modified double-pulley technique to create a double mattress construct. At the lateral side of the graft, the FiberTapes are shuttled through the 2 punch-holes.
Right shoulder. Lateral fixation of the graft is accomplished by means of a FiberTape SpeedBridge construct (Arthrex).
Similar articles
-
Superior Capsular Reconstruction: Fascia Lata Versus Acellular Dermal Allograft: A Systematic Review.Arthrosc Sports Med Rehabil. 2020 Jul 28;2(4):e389-e397. doi: 10.1016/j.asmr.2020.03.002. eCollection 2020 Aug. Arthrosc Sports Med Rehabil. 2020. PMID: 32875304 Free PMC article. Review.
-
Arthroscopic Single-Row Superior Capsular Reconstruction for Irreparable Rotator Cuff Tears.Arthrosc Tech. 2020 Apr 25;9(5):e675-e681. doi: 10.1016/j.eats.2020.01.024. eCollection 2020 May. Arthrosc Tech. 2020. PMID: 32489844 Free PMC article.
-
Superior Capsular Reconstruction With the Addition of an Acromial Acellular Dermal Allograft Spacer.Arthrosc Tech. 2018 Oct 22;7(11):e1181-e1190. doi: 10.1016/j.eats.2018.08.003. eCollection 2018 Nov. Arthrosc Tech. 2018. PMID: 30533367 Free PMC article.
-
Arthroscopic Superior Capsular Reconstruction With Acellular Dermal Allograft for the Treatment of Massive Irreparable Rotator Cuff Tears: Short-Term Clinical Outcomes and the Radiographic Parameter of Superior Capsular Distance.Arthroscopy. 2018 Jun;34(6):1764-1773. doi: 10.1016/j.arthro.2018.01.009. Epub 2018 Feb 15. Arthroscopy. 2018. PMID: 29456069
-
The role of Superior Capsule Reconstruction in the irreparable rotator cuff tear - A systematic review.Orthop Traumatol Surg Res. 2019 Dec;105(8):1535-1542. doi: 10.1016/j.otsr.2019.07.022. Epub 2019 Nov 11. Orthop Traumatol Surg Res. 2019. PMID: 31727588
Cited by
-
Superior Capsular Reconstruction: Fascia Lata Versus Acellular Dermal Allograft: A Systematic Review.Arthrosc Sports Med Rehabil. 2020 Jul 28;2(4):e389-e397. doi: 10.1016/j.asmr.2020.03.002. eCollection 2020 Aug. Arthrosc Sports Med Rehabil. 2020. PMID: 32875304 Free PMC article. Review.
-
Superior capsular reconstruction of the shoulder: the ABC (Arthroscopic Biceps Chillemi) technique.Eur J Orthop Surg Traumatol. 2018 Aug;28(6):1215-1223. doi: 10.1007/s00590-018-2183-1. Epub 2018 Mar 21. Eur J Orthop Surg Traumatol. 2018. PMID: 29564612
-
How to Use a Graft in Irreparable Rotator Cuff Tears: A Literature Review Update of Interposition and Superior Capsule Reconstruction Techniques.Curr Rev Musculoskelet Med. 2018 Mar;11(1):122-130. doi: 10.1007/s12178-018-9466-3. Curr Rev Musculoskelet Med. 2018. PMID: 29327176 Free PMC article. Review.
-
Arthroscopic Superior Capsule Reconstruction Using Autologous Fascia Lata and Biceps Tendon Augmentation.Arthrosc Tech. 2021 May 3;10(6):e1411-e1415. doi: 10.1016/j.eats.2021.02.004. eCollection 2021 Jun. Arthrosc Tech. 2021. PMID: 34258184 Free PMC article.
-
Arthroscopic superior capsular reconstruction with acellular human dermal allograft for irreparable rotator cuff tears: outcomes, complications, and reoperations at 2-year minimum follow-up.JSES Int. 2024 Dec 2;9(2):385-389. doi: 10.1016/j.jseint.2024.11.007. eCollection 2025 Mar. JSES Int. 2024. PMID: 40182267 Free PMC article.
References
-
- Denard P.J., Lädermann A., Brady P.C. Pseudoparalysis from a massive rotator cuff tear is reliably reversed with an arthroscopic rotator cuff repair in patients without preoperative glenohumeral arthritis. Am J Sports Med. 2015;43:2373–2378. - PubMed
-
- Denard P.J., Lädermann A., Jiwani A.Z., Burkhart S.S. Functional outcome after arthroscopic repair of massive rotator cuff tears in individuals with pseudoparalysis. Arthroscopy. 2012;28:1214–1219. - PubMed
-
- Denard P.J., Jiwani A.Z., Lädermann A., Burkhart S.S. Long-term outcome of arthroscopic massive rotator cuff repair: The importance of double-row fixation. Arthroscopy. 2012;28:909–915. - PubMed
-
- Burkhart S.S., Nottage W.M., Ogilvie-Harris D.J., Kohn H.S., Pachelli A. Partial repair of irreparable rotator cuff tears. Arthroscopy. 1994;10:363–370. - PubMed
-
- Mihata T., Lee T.Q., Watanabe C. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy. 2013;29:459–470. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
