

Acne and Rosacea
- PMID: 28150107
- PMCID: PMC5289119
- DOI: 10.1007/s13555-016-0168-8
Acne and Rosacea
Abstract
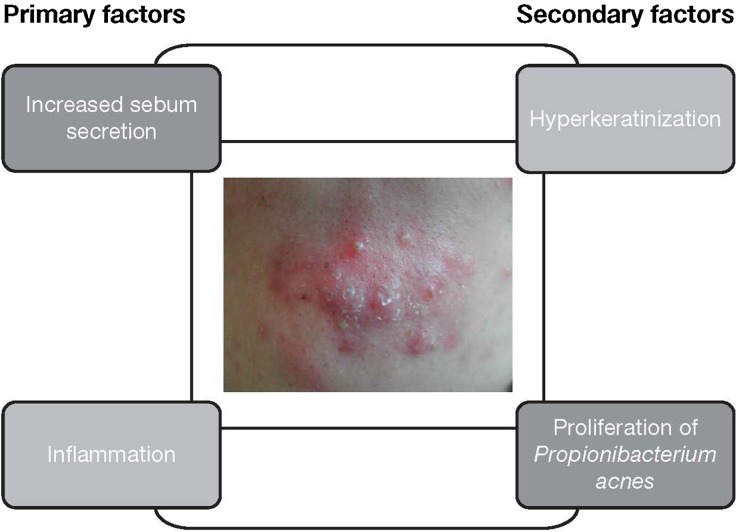
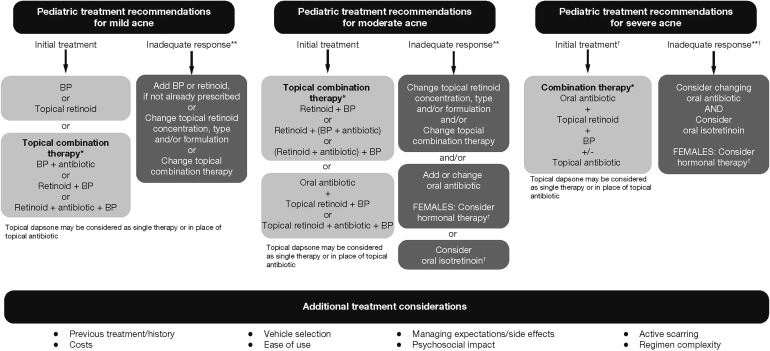
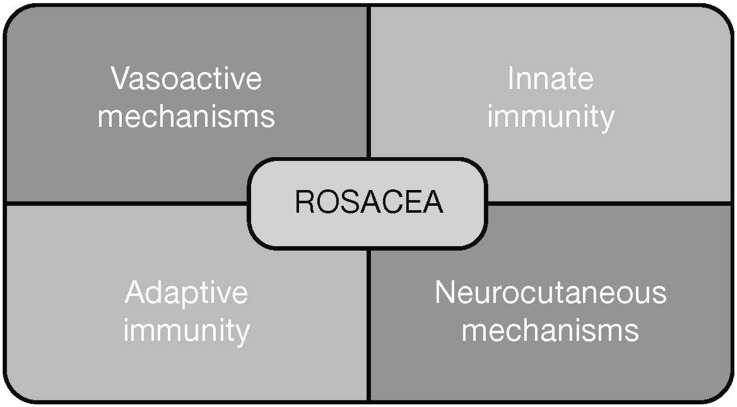
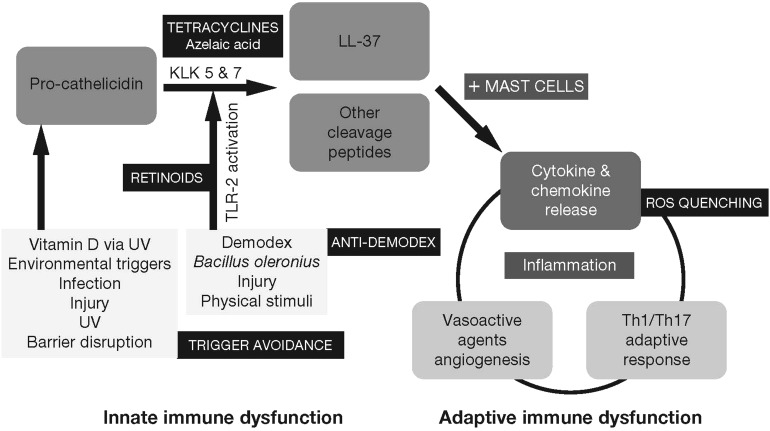
Acne, one of the most common skin diseases, affects approximately 85% of the adolescent population, and occurs most prominently at skin sites with a high density of sebaceous glands such as the face, back, and chest. Although often considered a disease of teenagers, acne is occurring at an increasingly early age. Rosacea is a chronic facial inflammatory dermatosis characterized by flushing (or transient facial erythema), persistent central facial erythema, inflammatory papules/pustules, and telangiectasia. Both acne and rosacea have a multifactorial pathology that is incompletely understood. Increased sebum production, keratinocyte hyper-proliferation, inflammation, and altered bacterial colonization with Propionibacterium acnes are considered to be the underlying disease mechanisms in acne, while the multifactorial pathology of rosacea is thought to involve both vasoactive and neurocutaneous mechanisms. Several advances have taken place in the past decade in the research field of acne and rosacea, encompassing pathogenesis and epidemiology, as well as the development of new therapeutic interventions. In this article, we provide an overview of current perspectives on the pathogenesis and treatment of acne and rosacea, including a summary of findings from recent landmark pathophysiology studies considered to have important implications for future clinical practice. The advancement of our knowledge of the different pathways and regulatory mechanisms underlying acne and rosacea is thought to lead to further advances in the therapeutic pipeline for both conditions, ultimately providing a greater array of treatments to address gaps in current management practices.
Keywords: Acne; Acne vulgaris; Adolescent; Pathogenesis; Pediatric; Pre-adolescent; Rosacea; Therapy.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
