

Comparison of two different size needles in endoscopic ultrasound-guided fine-needle aspiration for diagnosing solid pancreatic lesions: A meta-analysis of prospective controlled trials
- PMID: 28151856
- PMCID: PMC5293419
- DOI: 10.1097/MD.0000000000005802
Comparison of two different size needles in endoscopic ultrasound-guided fine-needle aspiration for diagnosing solid pancreatic lesions: A meta-analysis of prospective controlled trials
Abstract
Background: This meta-analysis aimed to provide a pooled analysis of prospective controlled trials comparing the diagnostic accuracy of 22-G and 25-G needles on endoscopic ultrasonography (EUS-FNA) of the solid pancreatic mass.
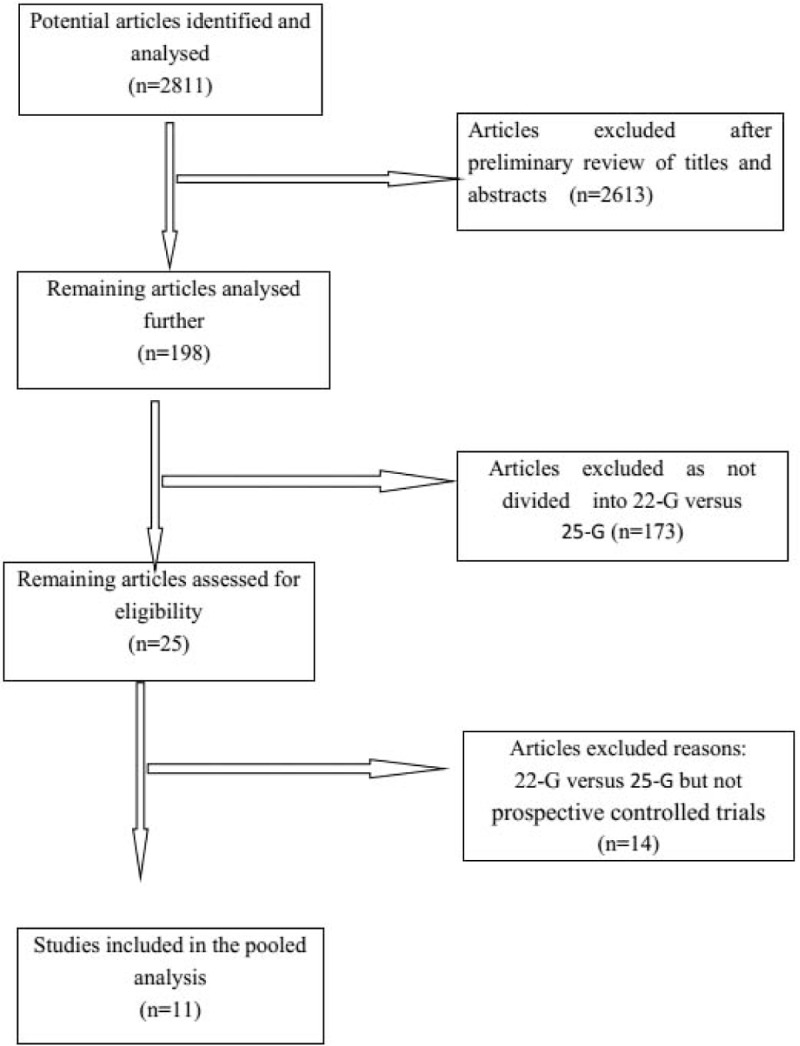
Methods: We established a rigorous study protocol according to Cochrane Collaboration recommendations. We systematically searched the PubMed and Embase databases to identify articles to include in the meta-analysis. Sensitivity, specificity, and corresponding 95% confidence intervals were calculated for 22-G and 25-G needles of individual studies from the contingency tables.
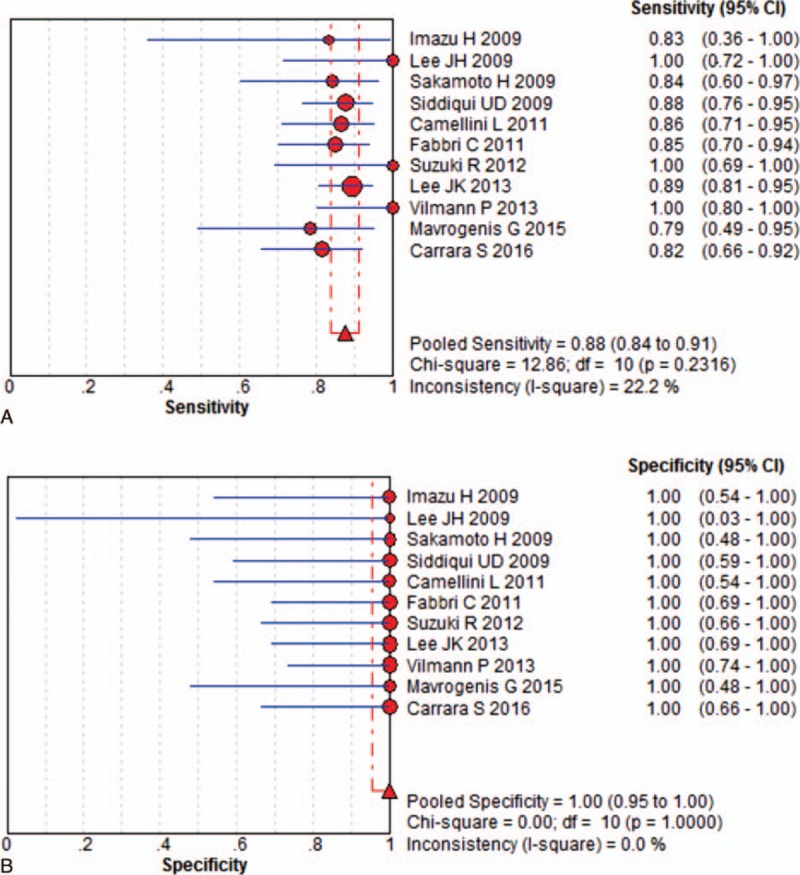
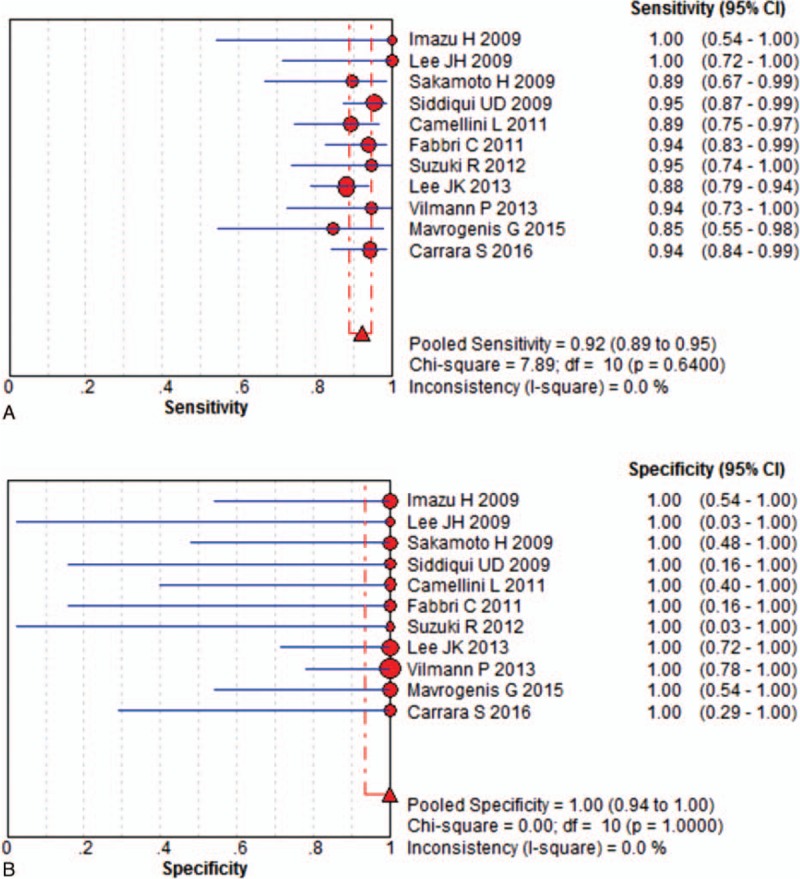
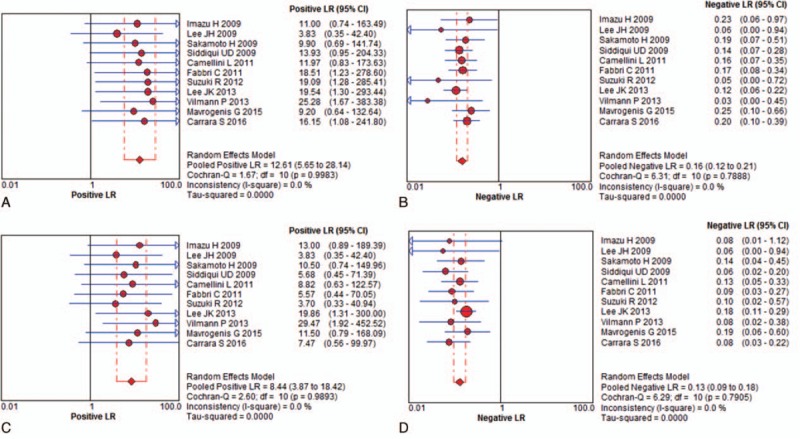
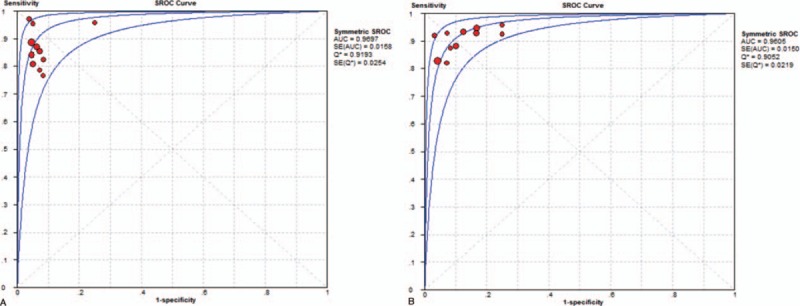
Results: Eleven prospective controlled trials included a total of 837 patients (412 with 22-G vs 425 with 25-G). Our outcomes revealed that 25-G needles (92% [95% CI, 89%-95%]) have higher sensitivity than 22-G needles (88% [95% CI, 84%-91%]) on solid pancreatic mass EUS-FNA (P = 0.046). However, there were no significant differences between the 2 groups in overall diagnostic specificity (P = 0.842). The pooled positive and negative likelihood ratio of the 22-G needle were 12.61 (95% CI, 5.65-28.14) and 0.16 (95% CI, 0.12-0.21), respectively. The pooled positive likelihood ratio was 12.61 (95% CI, 5.65-28.14), and the negative likelihood ratio was 0.16 (95% CI, 0.12-0.21) for the 22-G needle. The pooled positive likelihood ratio was 8.44 (95% CI, 3.87-18.42), and the negative likelihood ratio was 0.13 (95% CI, 0.09-0.18) for the 25-G needle. The area under the summary receiver operating characteristic curve was 0.97 for the 22-G needle and 0.96 for the 25-G needle.
Conclusion: Compared to the study of 22-G EUS-FNA needles, our study showed that 25-G needles have superior sensitivity in the evaluation of solid pancreatic lesions by EUS-FNA.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Cahn M, Chang K, Nguyen P, et al. Impact of endoscopic ultrasound with fine-needle aspiration on the surgical management of pancreatic cancer. Am J Surg 1996;172:470–2. - PubMed
-
- Erickson RA, Garza AA. Impact of endoscopic ultrasound on the management and outcome of pancreatic carcinoma. Am J Gastroenterol 2000;95:2248–54. - PubMed
-
- O’Toole D, Palazzo L, Arotcarena R, et al. Assessment of complications of EUS-guided fine-needle aspiration. Gastrointest Endosc 2001;53:470–4. - PubMed
-
- Kida M. Pancreatic masses. Gastrointest Endosc 2009;69(2 suppl):S102–9. - PubMed
-
- Itoi T, Tsuchiya T, Itokawa F, et al. Histological diagnosis by EUS-guided fine-needle aspiration biopsy in pancreatic solid masses without on-site cytopathologist: a single-center experience. Dig Endosc 2011;23(suppl 1):34–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
