

Impact of patient and treatment characteristics on glycemic control and hypoglycemia in patients with type 2 diabetes initiated to insulin glargine or NPH: A post hoc, pooled, patient-level analysis of 6 randomized controlled trials
- PMID: 28151905
- PMCID: PMC5293468
- DOI: 10.1097/MD.0000000000006022
Impact of patient and treatment characteristics on glycemic control and hypoglycemia in patients with type 2 diabetes initiated to insulin glargine or NPH: A post hoc, pooled, patient-level analysis of 6 randomized controlled trials
Abstract
Background: The goal of this post hoc analysis was to determine key patient and treatment-related factors impacting glycosylated hemoglobin (A1C) and hypoglycemia in patients with uncontrolled type 2 diabetes who were initiated to basal insulin (neutral protamine Hagedorn [NPH] or glargine).
Methods: Using individual patient-level data pooled from 6 treat-to-target trials, 2600 patients with type 2 diabetes on oral antidiabetic agents initiated to insulin glargine or NPH and treated for 24 to 36 weeks were analyzed.
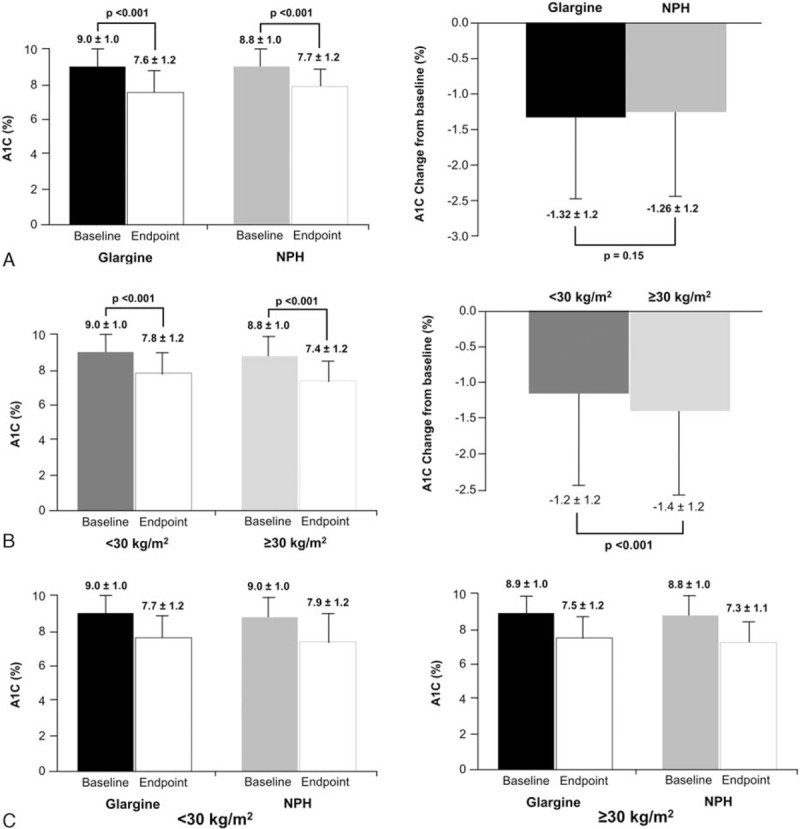
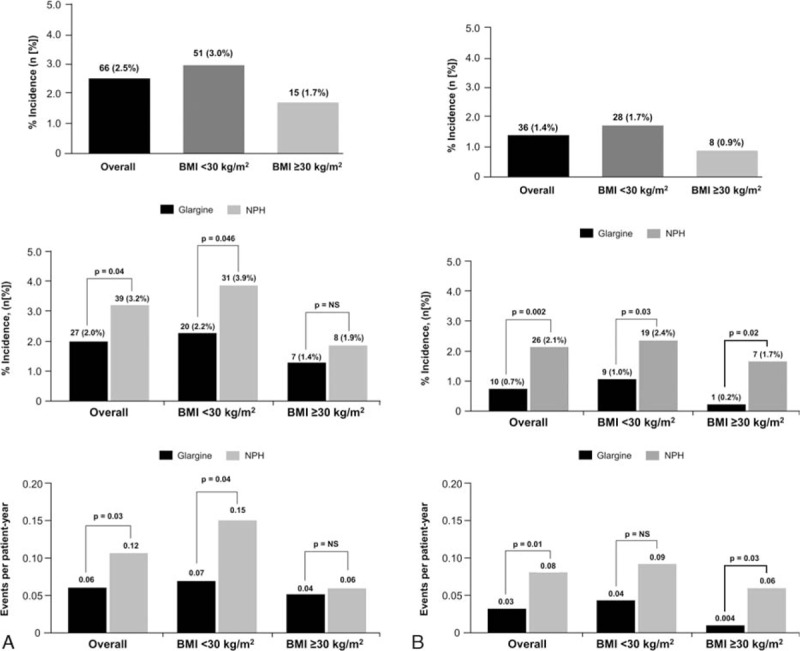
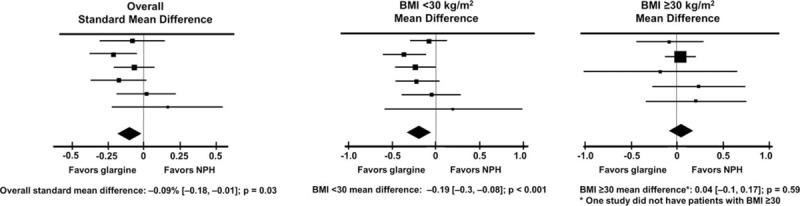
Results: Both treatments led to significant reduction in A1C levels compared with baseline, with no differences between treatment groups (mean ± standard deviation; glargine: -1.32 ± 1.2% vs NPH: -1.26 ± 1.2%; P = 0.15), with greater reduction in the BMI ≥30 kg/m group than in the BMI <30 kg/m group. Glargine reduced A1C significantly more than NPH in the BMI <30 kg/m group (-1.30 ± 1.18% vs -1.14 ± 1.22, respectively; P = 0.008), but not in the BMI ≥ 30 kg/m group (-1.37 ± 1.19 vs -1.48 ± 1.22, respectively; P = 0.18). Similar proportions of patients achieved A1C target of <7% (glargine 30.6%, NPH 29.1%; P = 0.39). Incidence of severe and severe nocturnal hypoglycemia was significantly lower in glargine versus NPH-treated patients (2.0% vs 3.9%; P = 0.04, and 0.7% vs 2.1%; P = 0.002, respectively), and occurred primarily in the BMI <30 kg/m group.
Conclusions: Initiation of basal insulin is highly effective in lowering A1C after oral antidiabetic agent failure. Glargine decreases A1C more than NPH in nonobese patients, and reduces the risk for severe and severe nocturnal hypoglycemia versus NPH both in obese and nonobese patients, but more so in nonobese patients. Thus, it is the nonobese patients who may benefit more from initiation of basal insulin as glargine than NPH.
Conflict of interest statement
Authors' contributions: JL also contributed to data collection for this manuscript. FP, PL, GBB, and CGF have no conflicts to disclose with regard to this post-hoc analysis. JL is a consultant to Sanofi. All authors contributed to the conduct, data analysis/interpretation, and writing of this manuscript. The authors report no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
