

Incidence and risk factors of adjacent segment disease following posterior decompression and instrumented fusion for degenerative lumbar disorders
- PMID: 28151909
- PMCID: PMC5293472
- DOI: 10.1097/MD.0000000000006032
Incidence and risk factors of adjacent segment disease following posterior decompression and instrumented fusion for degenerative lumbar disorders
Abstract
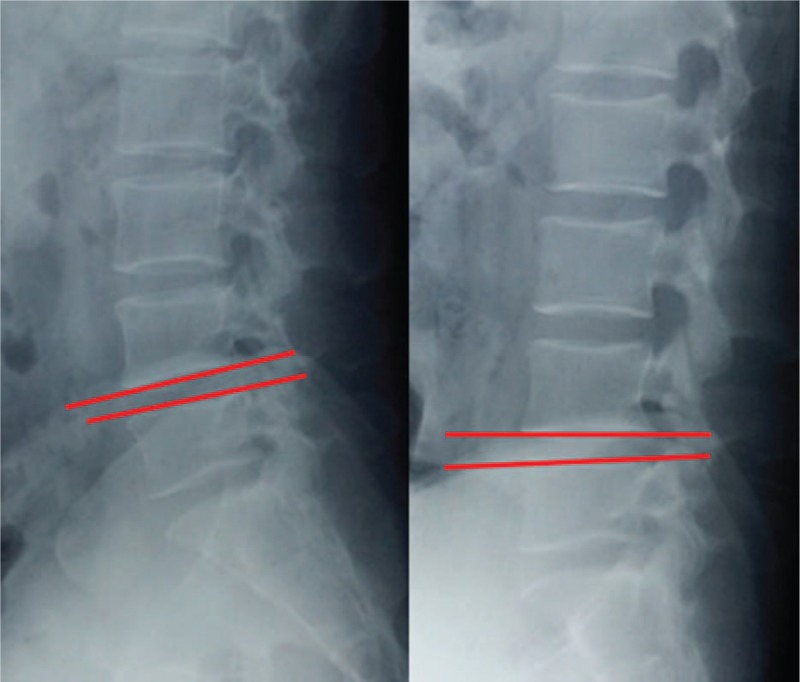
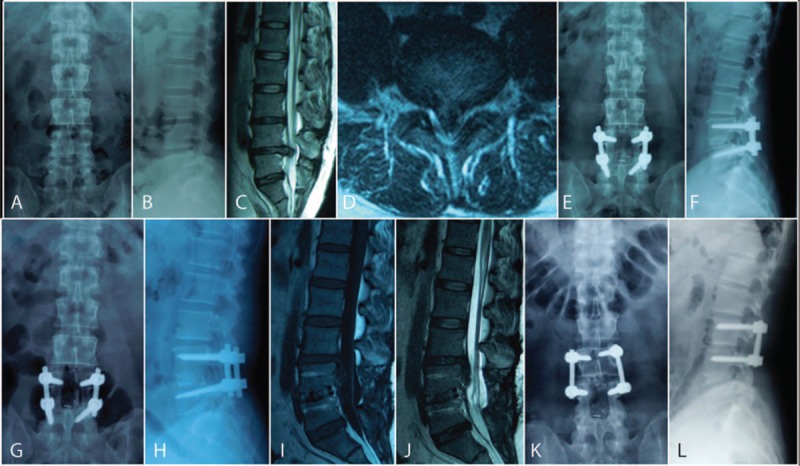
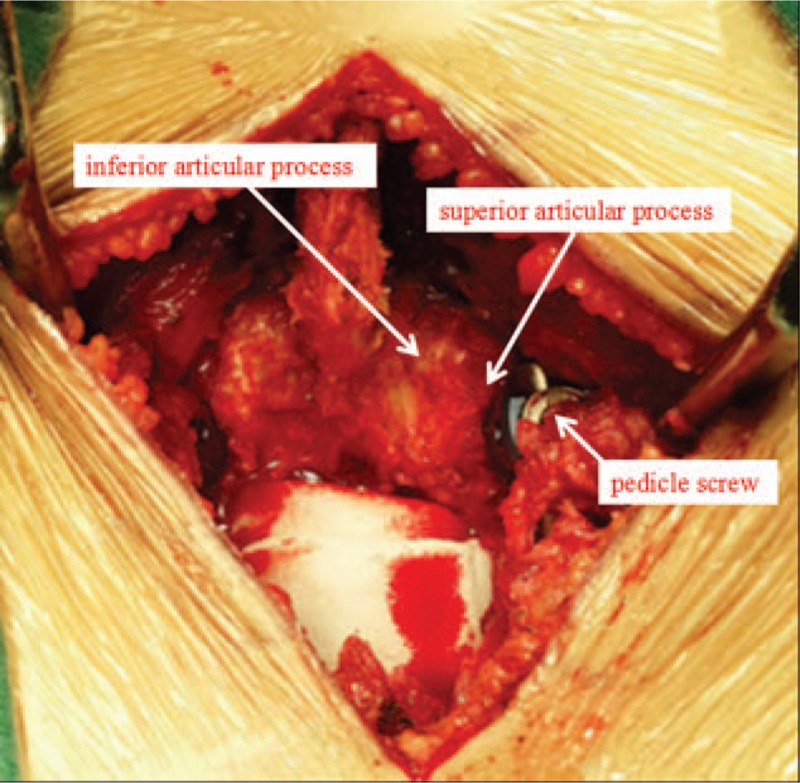
The purpose of this study was to explore incidence and risk factors of adjacent segment disease (ASD) following posterior decompression and instrumented fusion for degenerative lumbar disorders, and hope to provide references in decision making and surgical planning for both spinal surgeon and surgically treated patients.By retrieving the medical records from January 2011 to December 2013 in our hospital, 237 patients were retrospectively reviewed. According to the occurrence of ASD at follow up, patients were divided into 2 groups: ASD and N-ASD group. To investigate risk values for the occurrence of ASD, 3 categorized factors were analyzed statistically: Patient characteristics: age, sex, body mass index (BMI), bone mineral density (BMD), duration. Surgical variables: surgical strategy, number of fusion level, surgery segment, surgery time, blood loss, intraoperative superior facet joint violation. Radiographic parameters: preoperative lumbar lordosis, preoperative angular motion at adjacent segment, preoperative adjacent segment disc degeneration, preoperative paraspinal muscle degeneration.Postoperative ASD was developed in 15 of 237 patients (6.3%) at final follow up. There was no statistically significant difference between the 2 groups in patient characteristics of age, sex composition, BMD, duration, while the BMI was higher in ASD group than that in N-ASD group. There was no difference in surgical variables of surgical strategy, number of fusion level, surgery segment, surgery time, blood loss, while intraoperative superior facet joint violation was more common in ASD group than that in N-ASD group. There was no difference in radiographic parameters of preoperative lumbar lordosis, preoperative paraspinal muscle degeneration, while preoperative adjacent segment disc degeneration were more severe in ASD group than that in N-ASD group. The Logistic regression analysis revealed that, BMI >25 kg/m, preoperative disc degeneration, and superior facet joint violation were independently associated with ASD.In conclusion, higher BMI, preoperative disc degeneration at adjacent segment and intraoperative superior facet joint violation are risk factors for ASD. Patients who are overweight or obesity and with preoperative disc degeneration at adjacent segment should be fully informed the risk of ASD. For surgeons, it is essential to prevent superior facet joint violation in pedicle screw insertion procedure.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



Similar articles
-
Paraspinal muscle, facet joint, and disc problems: risk factors for adjacent segment degeneration after lumbar fusion.Spine J. 2016 Jul;16(7):867-75. doi: 10.1016/j.spinee.2016.03.010. Epub 2016 Mar 9. Spine J. 2016. PMID: 26970600
-
Adjacent segment disease after posterior lumbar instrumentation surgery for degenerative disease: Incidence and risk factors.J Orthop Surg (Hong Kong). 2019 May-Aug;27(2):2309499019842378. doi: 10.1177/2309499019842378. J Orthop Surg (Hong Kong). 2019. PMID: 31046589
-
Risk factors for adjacent segment disease requiring reoperation after posterior lumbar interbody fusion with screw fixation: focus on paraspinal muscle, facet joint, and disc degeneration.Acta Neurochir (Wien). 2022 Mar;164(3):913-922. doi: 10.1007/s00701-021-05073-x. Epub 2021 Dec 1. Acta Neurochir (Wien). 2022. PMID: 34850289
-
How to prevent preoperative adjacent segment degeneration L5/S1 segment occuring postoperative adjacent segment disease? A retrospective study of risk factor analysis.J Orthop Surg Res. 2025 Mar 10;20(1):259. doi: 10.1186/s13018-024-05439-8. J Orthop Surg Res. 2025. PMID: 40065447 Free PMC article. Review.
-
Demographic, Surgical, and Radiographic Risk Factors for Symptomatic Adjacent Segment Disease After Lumbar Fusion: A Systematic Review and Meta-Analysis.J Bone Joint Surg Am. 2021 Aug 4;103(15):1438-1450. doi: 10.2106/JBJS.20.00408. J Bone Joint Surg Am. 2021. PMID: 34166276
Cited by
-
Pedicle Screws and Facet Violation - The importance of the Angle between the Facet and the Screw.Rev Bras Ortop (Sao Paulo). 2020 Oct;55(5):642-648. doi: 10.1055/s-0040-1709200. Epub 2020 Jun 8. Rev Bras Ortop (Sao Paulo). 2020. PMID: 33093731 Free PMC article.
-
Will the adjustment of insertional pedicle screw positions affect the risk of adjacent segment diseases biomechanically? An in-silico study.Front Surg. 2023 Jan 12;9:1004642. doi: 10.3389/fsurg.2022.1004642. eCollection 2022. Front Surg. 2023. PMID: 36713678 Free PMC article.
-
Surgical risk factors associated with the development of adjacent segment pathology in the lumbar spine.EFORT Open Rev. 2021 Oct 19;6(10):966-972. doi: 10.1302/2058-5241.6.210050. eCollection 2021 Oct. EFORT Open Rev. 2021. PMID: 34760295 Free PMC article. Review.
-
Predictors of accurate intrapedicular screw placement in single-level lumbar (L4-5) fusion: robot-assisted pedicle screw, traditional pedicle screw, and cortical bone trajectory screw insertion.BMC Surg. 2022 Jul 24;22(1):284. doi: 10.1186/s12893-022-01733-6. BMC Surg. 2022. PMID: 35871659 Free PMC article.
-
Clinical outcomes of short rod technique in posterior lumbar interbody fusion surgery: a minimum of 2-year follow-up.Eur Spine J. 2024 Jan;33(1):339-355. doi: 10.1007/s00586-023-07950-8. Epub 2023 Nov 7. Eur Spine J. 2024. PMID: 37934266
References
-
- Rajaee SS, Bae HW, Kanim LE, et al. Spinal fusion in the United States: analysis of trends from 1998 to 2008. Spine (Phila Pa 1976) 2012;37:67–76. - PubMed
-
- Greenwood J, McGregor A, Jones F, et al. Rehabilitation following lumbar fusion surgery: a systematic review and meta-analysis. Spine (Phila Pa 1976) 2016;41:E28–36. - PubMed
-
- Tye EY, Alentado VJ, Mroz TE, et al. Comparison of clinical and radiographic outcomes in patients receiving single-level transforaminal lumbar interbody fusion with removal of unilateral or bilateral facet joints. Spine (Phila Pa 1976) 2016;41:E1039–45. - PubMed
-
- Bohl DD, Mayo BC, Massel DH, et al. Incidence and risk factors for pneumonia after posterior lumbar fusion procedures: an ACS-NSQIP study. Spine (Phila Pa 1976) 2016;41:1058–63. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
