

Clinical impact of pharmacogenetic profiling with a clinical decision support tool in polypharmacy home health patients: A prospective pilot randomized controlled trial
- PMID: 28151991
- PMCID: PMC5289536
- DOI: 10.1371/journal.pone.0170905
Clinical impact of pharmacogenetic profiling with a clinical decision support tool in polypharmacy home health patients: A prospective pilot randomized controlled trial
Abstract
Background: In polypharmacy patients under home health management, pharmacogenetic testing coupled with guidance from a clinical decision support tool (CDST) on reducing drug, gene, and cumulative interaction risk may provide valuable insights in prescription drug treatment, reducing re-hospitalization and emergency department (ED) visits. We assessed the clinical impact of pharmacogenetic profiling integrating binary and cumulative drug and gene interaction warnings on home health polypharmacy patients.
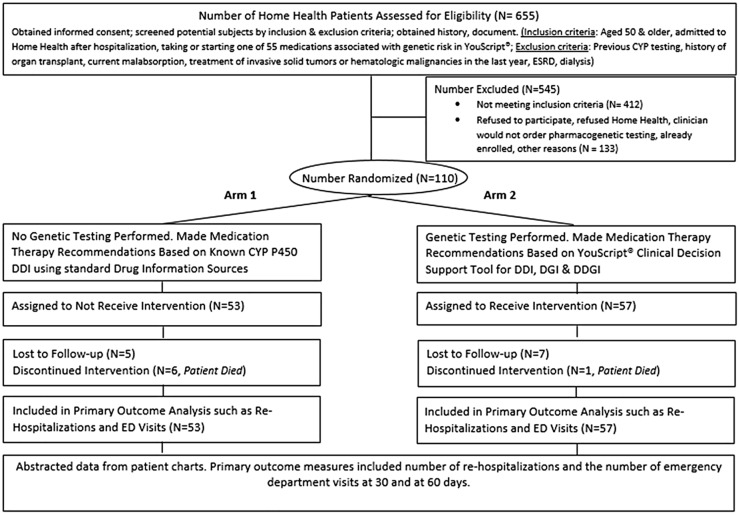
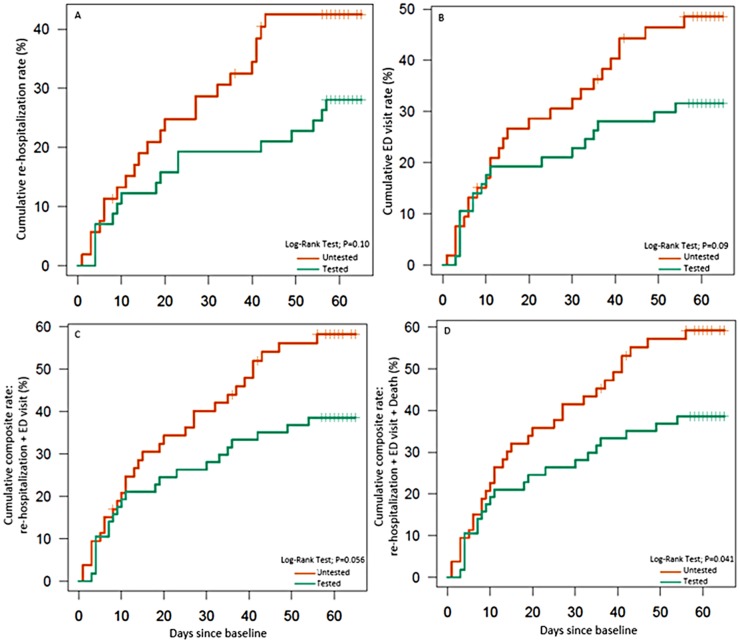
Methods and findings: This prospective, open-label, randomized controlled trial was conducted at one hospital-based home health agency between February 2015 and February 2016. Recruitment came from patient referrals to home health at hospital discharge. Eligible patients were aged 50 years and older and taking or initiating treatment with medications with potential or significant drug-gene-based interactions. Subjects (n = 110) were randomized to pharmacogenetic profiling (n = 57). The study pharmacist reviewed drug-drug, drug-gene, and cumulative drug and/or gene interactions using the YouScript® CDST to provide drug therapy recommendations to clinicians. The control group (n = 53) received treatment as usual including pharmacist guided medication management using a standard drug information resource. The primary outcome measure was the number of re-hospitalizations and ED visits at 30 and 60 days after discharge from the hospital. The mean number of re-hospitalizations per patient in the tested vs. untested group was 0.25 vs. 0.38 at 30 days (relative risk (RR), 0.65; 95% confidence interval (CI), 0.32-1.28; P = 0.21) and 0.33 vs. 0.70 at 60 days following enrollment (RR, 0.48; 95% CI, 0.27-0.82; P = 0.007). The mean number of ED visits per patient in the tested vs. untested group was 0.25 vs. 0.40 at 30 days (RR, 0.62; 95% CI, 0.31-1.21; P = 0.16) and 0.39 vs. 0.66 at 60 days (RR, 0.58; 95% CI, 0.34-0.99; P = 0.045). Differences in composite outcomes at 60 days (exploratory endpoints) were also found. Of the total 124 drug therapy recommendations passed on to clinicians, 96 (77%) were followed. These findings should be verified with additional prospective confirmatory studies involving real-world applications in larger populations to broaden acceptance in routine clinical practice.
Conclusions: Pharmacogenetic testing of polypharmacy patients aged 50 and older, supported by an appropriate CDST, considerably reduced re-hospitalizations and ED visits at 60 days following enrollment resulting in potential health resource utilization savings and improved healthcare.
Trial registration: ClinicalTrials.gov NCT02378220.
Conflict of interest statement
Competing Interests: We have the following interests: NAM, KCA and RKT are employees and potential equity holders of Genelex corporation. MBN is an employee of The Mountain-Whisper-Light Statistics. Genelex provided the support in the form of compensation for time for authors LSE and MBN. YouScript® is a clinical decision support tool with issued and pending patents. NAM is listed as an inventor on provisional patent application US 20160004838/WO 2016003514 A1, which relates to the drug interaction algorithm used by YouScript®. There are no further patents, products in development or marketed products to declare. This does not alter our adherence to all the PLOS ONE policies on sharing data and materials, as detailed online in the guide for authors.
Figures
References
-
- Home health care services: Assessing payment adequacy and updating payments. Medicare Payment Advisory Commission March 2015 Report to the Congress: Medicare Payment Policy. 2015;(March):213–36.
-
- Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533–43. - PubMed
-
- Evans WE, Relling MV. Pharmacogenomics: translating functional genomics into rational therapeutics. Science. 1999;286(5439):487–91. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
