

Survival Rates Using Individualized Bioselection Treatment Methods in Patients With Advanced Laryngeal Cancer
- PMID: 28152117
- PMCID: PMC5439146
- DOI: 10.1001/jamaoto.2016.3669
Survival Rates Using Individualized Bioselection Treatment Methods in Patients With Advanced Laryngeal Cancer
Abstract
Importance: Use of chemoradiotherapy for advanced laryngeal cancer led to a major shift in treatment as an alternative to laryngectomy. Despite widespread adoption of chemoradiotherapy, survival rates have not improved and the original premise of matching neoadjuvant chemotherapy tumor response to determine subsequent treatment has not been followed.
Objective: To determine whether improved survival could be achieved by incorporating a single cycle of neoadjuvant chemotherapy to select patients with advanced disease for either laryngectomy or concurrent chemoradiotherapy.
Design, setting, and participants: An unselected cohort of 247 patients with laryngeal cancer in an academic institution between 2002 and 2012 was evaluated. Patients with limited disease (stages I and II) underwent endoscopic resection, radiotherapy, or chemoradiotherapy for deeply invasive T2 lesions. For patients with advanced disease (stages III and IV), neoadjuvant chemotherapy, concurrent chemoradiotherapy, or primary surgery was recommended. Overall survival (OS) and disease-specific survival (DSS) were analyzed. Median follow-up was 48 months. The study was conducted from January 1, 2002, to December 31, 2012; data analysis was completed December 1, 2015.
Interventions: Endoscopic resection, radiotherapy, chemoradiotherapy, neoadjuvant chemotherapy, concurrent chemoradiotherapy, and primary surgery.
Main outcomes and measures: Overall survival and DSS.
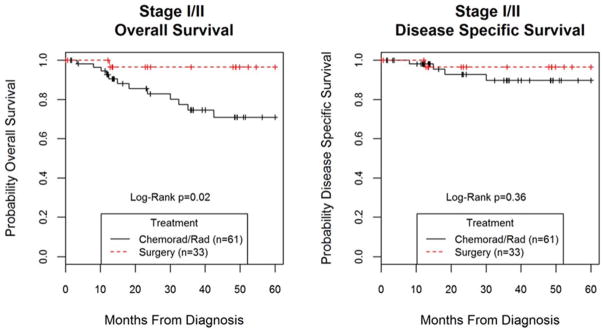
Results: Of the 247 patients, 191 (77.3%) were male; mean (SD) age was 59.6 (10.4) years. Of 94 patients with limited disease, 33 (35.1%) underwent endoscopic resection; 50 (53.2%), radiotherapy alone; and 11 (11.7%), chemoradiotherapy for deeply invasive T2 lesions. Of 153 patients with advanced disease, 71 (46.4%) received neoadjuvant chemotherapy; 50 (32.7%), concurrent chemoradiotherapy; and 32 (20.9%), surgery. Five-year OS and DSS was 75% (95% CI, 68%-81%) and 83% (95% CI, 77%-88%), respectively, for the entire cohort. The DSS was 92% (95% CI, 83%-97%) for patients with stage I or II and 78% (95% CI, 69%-84%) for patients with stage III or IV disease. For patients with advanced disease, 5-year OS and DSS ranged from 78% (95% CI, 55%-90%) and 91% (95% CI, 67%-98%), respectively, for surgery; to 76% (95% CI, 63%-85%) and 79% (95% CI, 67%-88%), respectively, for neoadjuvant bioselection; and to 61% (95% CI, 44%-75%) and 66% (95% CI, 48%-79%), respectively, for primary chemoradiotherapy. Propensity-adjusted, multivariable controlling for known prognostic factors DSS was significantly improved in the neoadjuvant group compared with the chemoradiotherapy group (hazard ratio [HR], 0.48; 95% CI, 0.29-0.80).
Conclusions and relevance: Superior survival rates were achieved with a bioselective treatment approach using a single cycle of neoadjuvant chemotherapy. Good survival rates were also achieved in patients selected for primary surgery, and both neoadjuvant chemotherapy and primary surgery were better than survival rates with concurrent chemoradiotherapy, suggesting that the optimal individualized treatment approach for patients with advanced laryngeal cancer has not yet been defined.
Figures




Comment in
-
Individualized Treatment of Laryngeal Cancer.JAMA Otolaryngol Head Neck Surg. 2017 Apr 1;143(4):367. doi: 10.1001/jamaoto.2016.4298. JAMA Otolaryngol Head Neck Surg. 2017. PMID: 28152132 No abstract available.
References
-
- Hoffman HT, Porter K, Karnell LH, Cooper JS, Weber RS, Langer CJ, Ang KK, Gay G, Stewart A, Robinson RA. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006 Sep;116(9 Pt 2 Suppl 111):1–13. - PubMed
-
- Chen AY, Halpern M. Factors predictive of survival in advanced laryngeal cancer. Arch Otolaryngol Head Neck Surg. 2007 Dec;133(12):1270–6. - PubMed
-
- Megwalu U, Sikora A. Survival outcomes in advanced laryngeal cancer. JAMA Otolaryngol Head Neck Surg. 2014;140:855–860. - PubMed
-
- Surveillance, Epidemiology and End Results Program (SEER) of the National Cancer Institute. http://seer.cancer.gov/statfacts/html/laryn.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
