

Population-Attributable Risk Proportion of Clinical Risk Factors for Breast Cancer
- PMID: 28152151
- PMCID: PMC5540816
- DOI: 10.1001/jamaoncol.2016.6326
Population-Attributable Risk Proportion of Clinical Risk Factors for Breast Cancer
Erratum in
-
Errors in Statistical Programming.JAMA Oncol. 2019 Nov 1;5(11):1643. doi: 10.1001/jamaoncol.2019.4065. JAMA Oncol. 2019. PMID: 31556906 Free PMC article. No abstract available.
Abstract
Importance: Many established breast cancer risk factors are used in clinical risk prediction models, although the proportion of breast cancers explained by these factors is unknown.
Objective: To determine the population-attributable risk proportion (PARP) for breast cancer associated with clinical breast cancer risk factors among premenopausal and postmenopausal women.
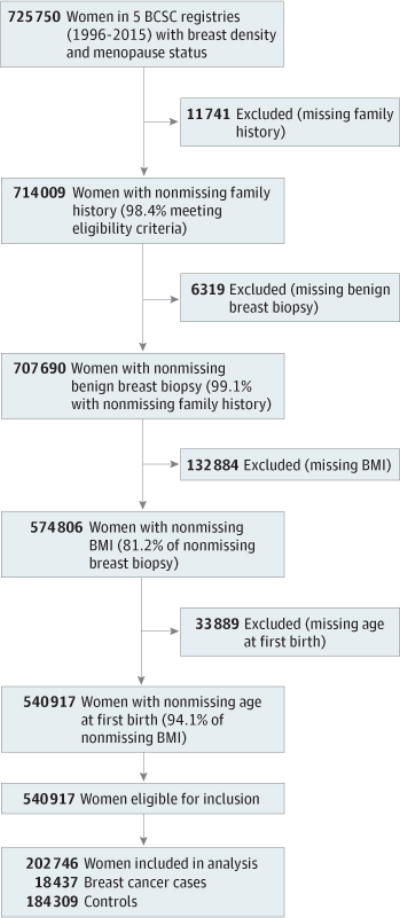
Design, setting, and participants: Case-control study with 1:10 matching on age, year of risk factor assessment, and Breast Cancer Surveillance Consortium (BCSC) registry. Risk factor data were collected prospectively from January 1, 1996, through October 31, 2012, from BCSC community-based breast imaging facilities. A total of 18 437 women with invasive breast cancer or ductal carcinoma in situ were enrolled as cases and matched to 184 309 women without breast cancer, with a total of 58 146 premenopausal and 144 600 postmenopausal women enrolled in the study.
Exposures: Breast Imaging Reporting and Data System (BI-RADS) breast density (heterogeneously or extremely dense vs scattered fibroglandular densities), first-degree family history of breast cancer, body mass index (>25 vs 18.5-25), history of benign breast biopsy, and nulliparity or age at first birth (≥30 years vs <30 years).
Main outcomes and measures: Population-attributable risk proportion of breast cancer.
Results: Of the 18 437 women with breast cancer, the mean (SD) age was 46.3 (3.7) years among premenopausal women and 61.7 (7.2) years among the postmenopausal women. Overall, 4747 (89.8%) premenopausal and 12 502 (95.1%) postmenopausal women with breast cancer had at least 1 breast cancer risk factor. The combined PARP of all risk factors was 52.7% (95% CI, 49.1%-56.3%) among premenopausal women and 54.7% (95% CI, 46.5%-54.7%) among postmenopausal women. Breast density was the most prevalent risk factor for both premenopausal and postmenopausal women and had the largest effect on the PARP; 39.3% (95% CI, 36.6%-42.0%) of premenopausal and 26.2% (95% CI, 24.4%-28.0%) of postmenopausal breast cancers could potentially be averted if all women with heterogeneously or extremely dense breasts shifted to scattered fibroglandular breast density. Among postmenopausal women, 22.8% (95% CI, 18.3%-27.3%) of breast cancers could potentially be averted if all overweight and obese women attained a body mass index of less than 25.
Conclusions and relevance: Most women with breast cancer have at least 1 breast cancer risk factor routinely documented at the time of mammography, and more than half of premenopausal and postmenopausal breast cancers are explained by these factors. These easily assessed risk factors should be incorporated into risk prediction models to stratify breast cancer risk and promote risk-based screening and targeted prevention efforts.
Conflict of interest statement
Figures
References
-
- Amir E, Freedman OC, Seruga B, Evans DG. Assessing women at high risk of breast cancer: a review of risk assessment models. J Natl Cancer Inst. 2010;102(10):680–691. - PubMed
-
- Kopans DB. An open letter to panels that are deciding guidelines for breast cancer screening. Breast Cancer Res Treat. 2015;151(1):19–25. - PubMed
-
- Trentham-Dietz A, Kerlikowske K, Stout NK, et al. Breast Cancer Surveillance Consortium and the Cancer Intervention and Surveillance Modeling Network Tailoring breast cancer screening intervals by breast density and risk for women aged 50 years or older: collaborative modeling of screening outcomes. Ann Intern Med. 2016;165(10):700–712. - PMC - PubMed
-
- Nelson HD, Smith ME, Griffin JC, Fu R. Use of medications to reduce risk for primary breast cancer: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2013;158(8):604–614. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
