

Imaging near orthopedic hardware
- PMID: 28152257
- PMCID: PMC5464983
- DOI: 10.1002/jmri.25577
Imaging near orthopedic hardware
Abstract
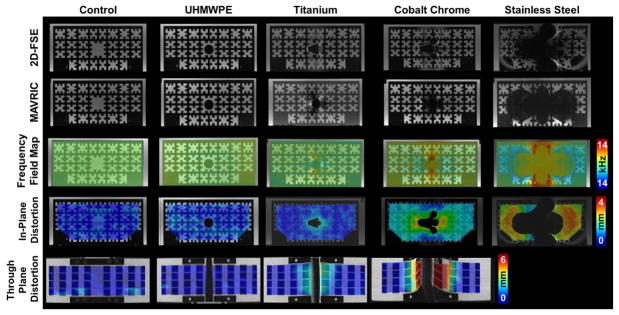
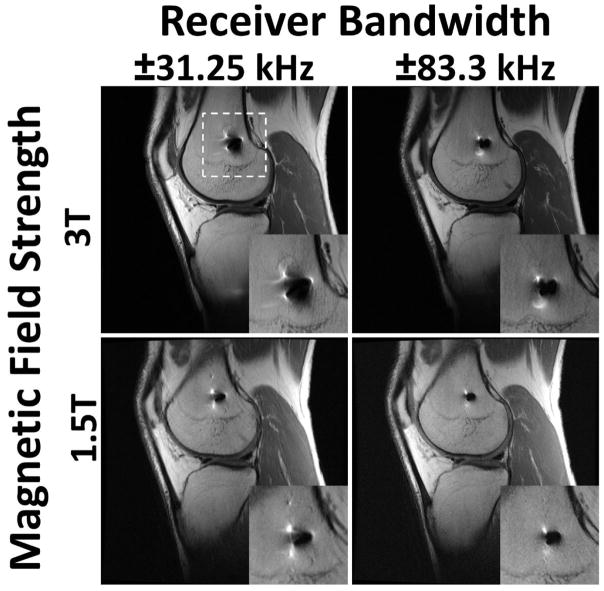
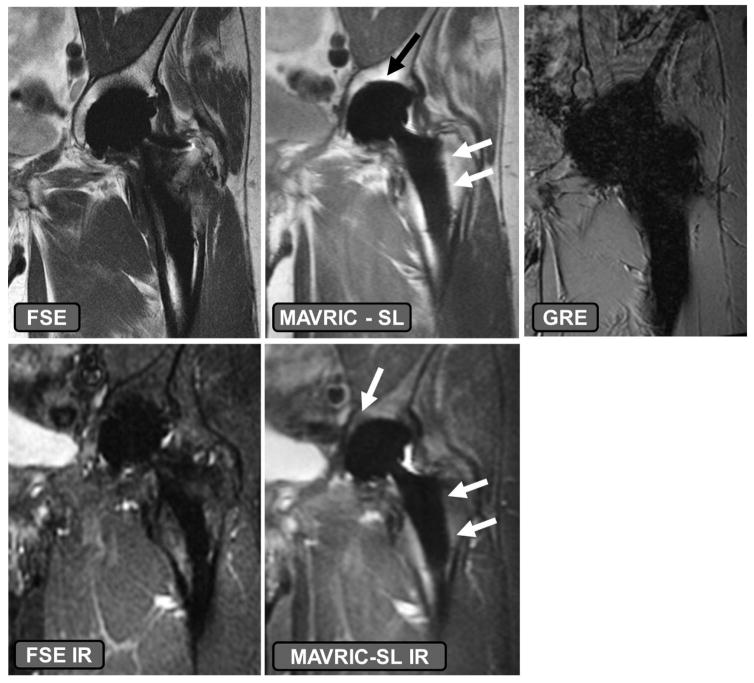
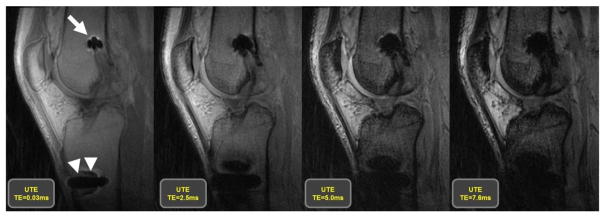
Over one million total joint replacement surgeries were performed in the US in 2013 alone, and this number is expected to more than double by 2030. Traditional imaging techniques for postoperative evaluation of implanted devices, such as radiography, computerized tomography, or ultrasound, utilize ionizing radiation, suffer from beam hardening artifact, or lack the inherent high contrast necessary to adequately evaluate soft tissues around the implants, respectively. Magnetic resonance imaging (MRI), due to its ability to generate multiplanar, high-contrast images without the use of ionizing radiation is ideal for evaluating periprosthetic soft tissues but has traditionally suffered from in-plane and through-plane data misregistration due to the magnetic susceptibility of implanted materials. A recent renaissance in the interest of imaging near arthroplasty and implanted orthopedic hardware has led to the development of new techniques that help to mitigate the effects of magnetic susceptibility. This article describes the challenges of performing imaging near implanted orthopedic hardware, how to generate clinically interpretable images when imaging near implanted devices, and how the images may be interpreted for clinical use. We will also describe current developments of utilizing MRI to evaluate implanted orthopedic hardware.
Level of evidence: 3 Technical Efficacy: Stage 2 J. MAGN. RESON. IMAGING 2017;46:24-39.
Keywords: MRI; arthroplasty; metal; susceptibility.
© 2017 International Society for Magnetic Resonance in Medicine.
Figures
References
-
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223. - PubMed
-
- Koopman WJ. Arthritis and Allied Conditions: A Textbook of Rheumatology. 13. Vol. 1. Williams & Wilkins; Baltimore: 1997.
-
- Centers for Disease Control. Prevalence and most common causes of disability among adults—United States, 2005. Morbidity and Mortality Weekly Report. 2009;58:421–426. - PubMed
-
- Agency for Healthcare Research and Quality. [Accessed 29 Sept, 2016];HCUPnet, Healthcare Cost and Utilization Project. https://www.hcup-us.ahrq.gov/
-
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. JBJS Am. 2007;89:780–785. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
