

Qualifiers of atypia in the cytologic diagnosis of thyroid nodules are associated with different Afirma gene expression classifier results and clinical outcomes
- PMID: 28152275
- PMCID: PMC5484344
- DOI: 10.1002/cncy.21827
Qualifiers of atypia in the cytologic diagnosis of thyroid nodules are associated with different Afirma gene expression classifier results and clinical outcomes
Abstract
Background: Thyroid nodules with atypia of undetermined significance (AUS) on fine-needle aspiration (FNA) have a low risk of malignancy that appears to vary based on specific features described in the AUS diagnosis. The Afirma gene expression classifier (GEC) is a molecular test designed to improve preoperative risk stratification of thyroid nodules, but its performance for different patterns of AUS has not been defined. The objective of this study was to assess GEC results and clinical outcomes in AUS nodules with architectural atypia (AUS-A), cytologic atypia (AUS-C) or both (AUS-C/A).
Methods: This was a retrospective review of all thyroid nodules with AUS cytopathology that underwent GEC testing at the authors' institution over a period of >4 years.
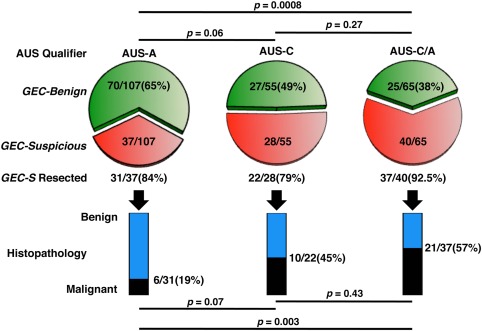
Results: In 227 nodules that had AUS cytology results and Afirma GEC testing, the rate of benign GEC results was higher in AUS-A nodules (70 of 107; 65%) than in AUS-C/A nodules (25 of 65; 38%; P = .0008), and AUS-C nodules exhibited an intermediate rate of benign results (27 of 55 nodules; 59%). The risk of cancer among patients who had GEC-suspicious nodules, 86% of whom underwent resection, was 19% (6 of 25) for AUS-A nodules compared with 57% (21 of 37) for AUS-C/A nodules (P = .003) and 45% (10 of 22) for AUS-C nodules (P = .07). In nodules that had an indeterminate repeat cytology result, no difference was observed in the rate of benign GEC results or in the malignancy rate compared with nodules that had a single cytology result.
Conclusions: The performance characteristics of Afirma GEC testing vary, depending on qualifiers of cytologic atypia. Recognition of these differences may enable clinicians to provide improved counseling and treatment recommendations to patients. Cancer Cytopathol 2017;125:313-322. © 2017 American Cancer Society.
Keywords: Afirma gene expression classifier; architectural atypia; atypia of undetermined significance (AUS); cytologic atypia; cytology; follicular lesion of undetermined significance (FLUS); indeterminate cytology; thyroid nodule.
© 2017 The Authors. Cancer Cytopathology published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Figures
Similar articles
-
UTILITY OF ULTRASOUND VERSUS GENE EXPRESSION CLASSIFIER IN THYROID NODULES WITH ATYPIA OF UNDETERMINED SIGNIFICANCE.Endocr Pract. 2016 Oct;22(10):1199-1203. doi: 10.4158/EP161231.OR. Epub 2016 Jul 13. Endocr Pract. 2016. PMID: 27409819
-
The impact of noninvasive follicular thyroid neoplasm with papillary-like nuclear features on the performance of the Afirma gene expression classifier.Cancer Cytopathol. 2017 Sep;125(9):683-691. doi: 10.1002/cncy.21879. Epub 2017 May 24. Cancer Cytopathol. 2017. PMID: 28544601
-
Noninvasive Follicular Variant of Papillary Thyroid Carcinoma and the Afirma Gene-Expression Classifier.Thyroid. 2016 Jul;26(7):911-5. doi: 10.1089/thy.2015.0644. Thyroid. 2016. PMID: 27219469
-
Follow-up of atypia and follicular lesions of undetermined significance in thyroid fine needle aspiration cytology.Cytopathology. 2013 Dec;24(6):385-90. doi: 10.1111/cyt.12021. Epub 2012 Oct 18. Cytopathology. 2013. PMID: 23078633 Review.
-
High risk of malignancy in cases with atypia of undetermined significance on fine needle aspiration of thyroid nodules even after exclusion of NIFTP.Diagn Cytopathol. 2020 Nov;48(11):986-997. doi: 10.1002/dc.24533. Epub 2020 Aug 3. Diagn Cytopathol. 2020. PMID: 32745375
Cited by
-
Assessing Bias and Limitations of Clinical Validation Studies of Molecular Diagnostic Tests for Indeterminate Thyroid Nodules: Systematic Review and Meta-Analysis.Thyroid. 2022 Oct;32(10):1144-1157. doi: 10.1089/thy.2022.0269. Epub 2022 Sep 26. Thyroid. 2022. PMID: 35999710 Free PMC article.
-
Extending expressed RNA genomics from surgical decision making for cytologically indeterminate thyroid nodules to targeting therapies for metastatic thyroid cancer.Cancer Cytopathol. 2019 Jun;127(6):362-369. doi: 10.1002/cncy.22132. Epub 2019 Apr 24. Cancer Cytopathol. 2019. PMID: 31017745 Free PMC article.
-
Performance of Afirma genomic sequencing classifier and histopathological outcome are associated with patterns of atypia in Bethesda category III thyroid nodules.Cancer Cytopathol. 2022 Nov;130(11):891-898. doi: 10.1002/cncy.22625. Epub 2022 Jul 5. Cancer Cytopathol. 2022. PMID: 35789120 Free PMC article.
-
Genetic testing for indeterminate thyroid cytology: review and meta-analysis.Endocr Relat Cancer. 2018 Mar;25(3):R163-R177. doi: 10.1530/ERC-17-0405. Epub 2017 Dec 18. Endocr Relat Cancer. 2018. PMID: 29255094 Free PMC article.
-
Atypia of undetermined significance/follicular lesions of undetermined significance: What radiologists need to know.Neuroradiol J. 2021 Apr;34(2):70-79. doi: 10.1177/1971400920983566. Epub 2020 Dec 28. Neuroradiol J. 2021. PMID: 33369519 Free PMC article. Review.
References
-
- Yassa L, Cibas ES, Benson CB, et al. Long‐term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer. 2007;111:508–516. - PubMed
-
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133. - PMC - PubMed
-
- Gharib H, Papini E, Paschke R, et al; AACE/AME/ETA Task Force on Thyroid Nodules . American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: executive summary of recommendations. J Endocrinol Invest. 2010;33:51–56. - PubMed
-
- Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid. 2009;19:1159–1165. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
