

Case Reports
doi: 10.2169/internalmedicine.56.7422.
Epub 2017 Feb 1.
Pancreatic Fistula Extending into the Thigh Caused by the Rupture of an Intraductal Papillary Mucinous Adenoma of the Pancreas
Affiliations
- PMID: 28154275
- PMCID: PMC5348455
- DOI: 10.2169/internalmedicine.56.7422
Item in Clipboard
Case Reports
Pancreatic Fistula Extending into the Thigh Caused by the Rupture of an Intraductal Papillary Mucinous Adenoma of the Pancreas
Intern Med.
2017.
Abstract
We herein report the first case of a pancreatic fistula extending into the thigh caused by the rupture of an intraductal papillary mucinous neoplasm (IPMN) of the pancreas. An 80-year-old man was suspected to have necrotizing fasciitis because of right femoral pain. Computed tomography showed fluid retention from the pancreatic head to the right iliopsoas muscle and an IPMN at the pancreatic head. The findings of endoscopic retrograde pancreatography led to the suspicion of a minor leak and a pancreatic stent was placed. The patient died due to an uncontrollable infection. A pathological autopsy showed a pancreatic fistula extending into the thigh that had been caused by the rupture of the IPMN.
Figures

A picture of the right femoral region on admission. After a tentative incision was made, redness and swelling were observed in the right femoral region.
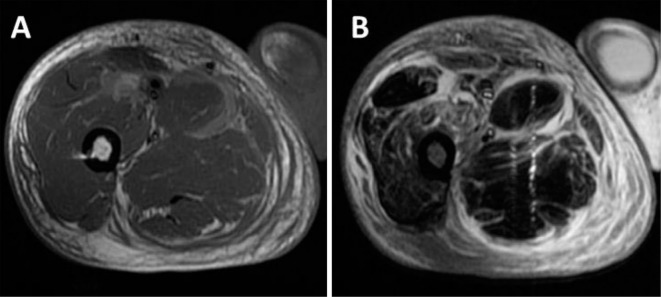
Magnetic resonance images. A: A T1-weighted image, showing moderate-to-high signal intensity around the muscle. B: A fat-suppressed T2-weighted image, showing high signal intensity in the quadriceps femoris muscle, the gracilis muscle, and the semimembranosus muscle.
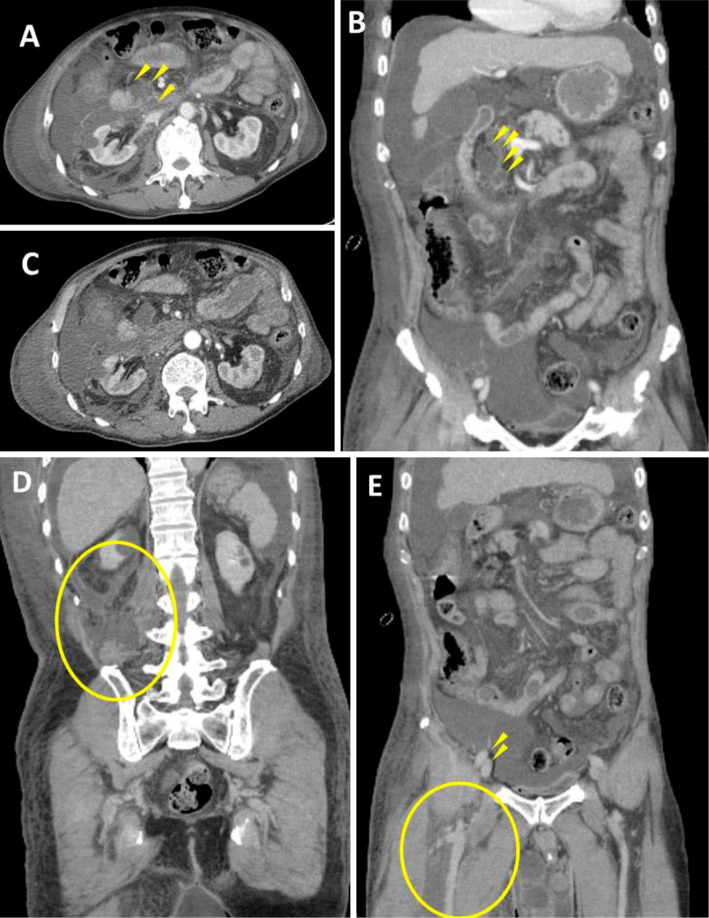
Abdominal contrast-enhanced computed tomographic scans. A, B: Atrophy and degeneration associated with a lack of parenchyma were observed in part of the uncinate process and the body of the pancreas. A good contrast effect was obtained in the pancreas. Cystic lesions were present in the uncinate process of the pancreas (arrowheads). C, D: Fluid retention extended from the duodenum to the right anterior pararenal space, the perirenal space, and the posterior pararenal space (circle). E: Fluid retention (circle) extended to the thigh over the ilium at the level of the femoral artery and vein (arrowheads).
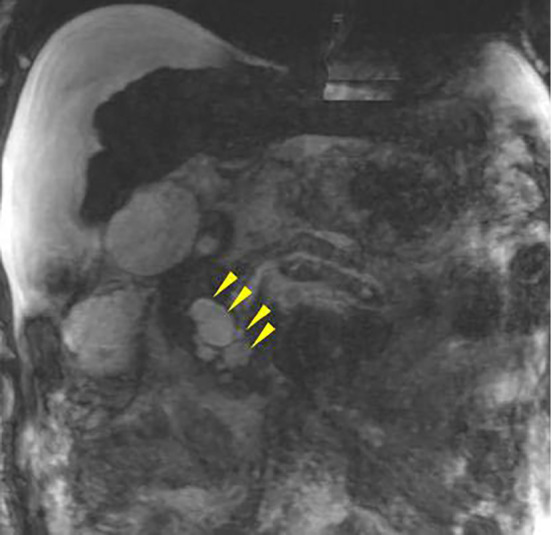
Magnetic resonance cholangiopancreatography. Cystic lesions were present in the uncinate process of the pancreas (arrowheads). This image was not clear because of an artifact and the presence of a large amount of ascites.
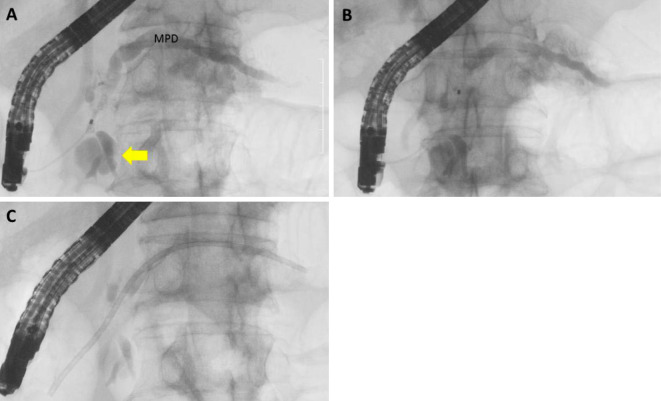
The endoscopic retrograde pancreatographic findings. A: Pancreatography showed the cystic dilation of a branch of the pancreatic duct at the head of the pancreas (arrow). The entire main pancreatic duct was dilated. Mild stricture was found in the main pancreatic duct at the head of the pancreas. B: Although we could not find an obvious leak from the pancreatic ducts, the contrast medium washed out quickly. C: Endoscopic pancreatic sphincterotomy was performed and a 7-French, 12-cm pancreatic stent was placed in the main pancreatic duct.
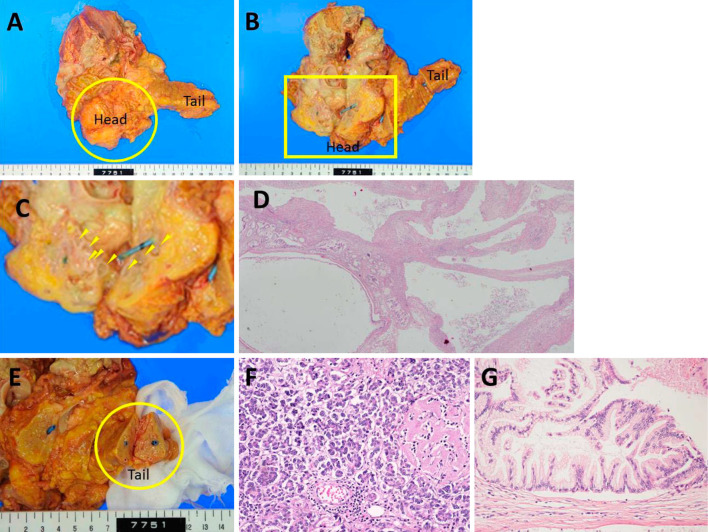
The pathological findings. A: An elastic soft mass (6×8×5 cm, circle) extended from the pancreatic head and surrounded Gerota’s fascia of the right kidney. B: The cut surface of the pancreatic head showed the presence of cystic lesions of various sizes, with the leakage of milky-white viscous fluid (arrowhead). The rupture point of the IPMN could not be located due to the presence of inflammation, necrosis, and fibrosis. A pancreatic stent had been placed in the main pancreatic duct. C: An enlarged view of the square area of B. D (×20): The histological findings of pancreatic head showed the presence of cystic lesions of various sizes. E: Macroscopic findings showed that the structures of the tail (circle) of the pancreas were relatively well preserved. F (×200): The histological findings showed that the acinar structures of the tail of the pancreas were relatively well preserved; small regions of fat necrosis were sporadically found and hyalinization of the islets of Langerhans had occurred due to diabetes mellitus. No fibrosis was found in the tail of the pancreas. The macroscopic and histological findings showed that there was no obvious chronic pancreatitis. G (×200): Atypical papillary proliferation was found in some of the cystic lesions at the pancreatic head, indicating the presence of an intraductal papillary mucinous adenoma (IPMA) of the pancreas.
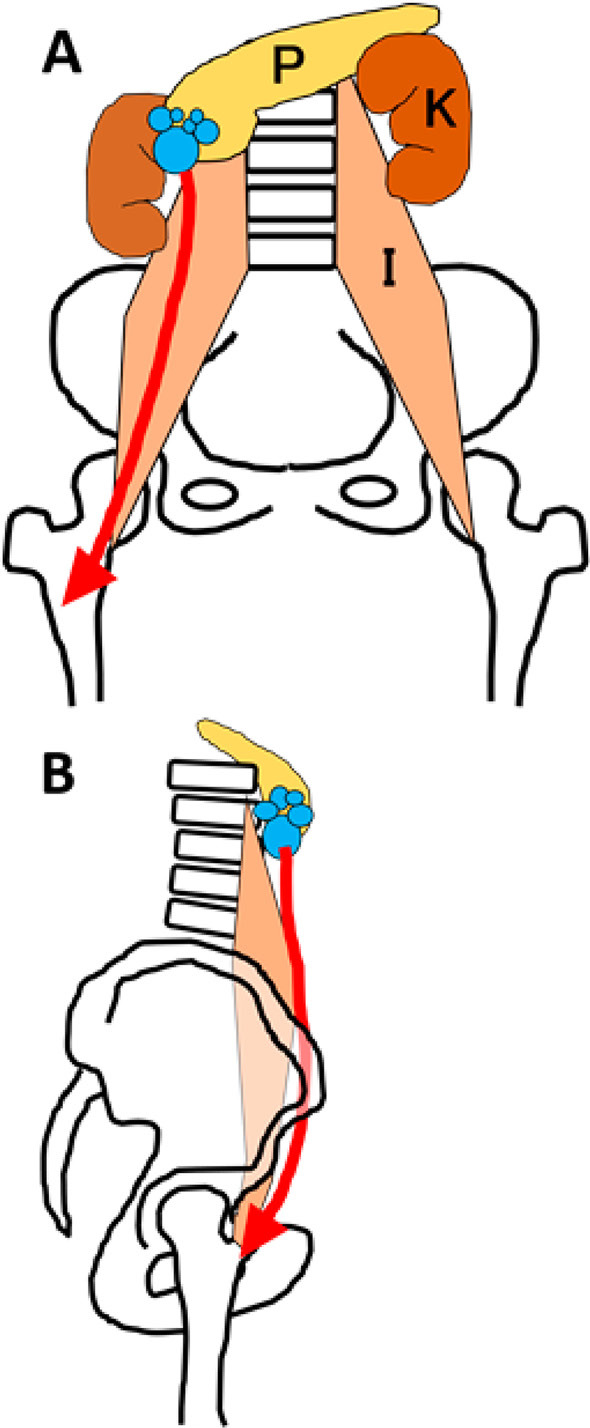
A schematic illustration of the pancreatic fistula extending into the right thigh. The leaked pancreatic juice might have passed through the retroperitoneum and moved along the right kidney and the iliopsoas muscle to arrive at the thigh. A: Frontal view. B: Lateral view. (P: pancreas, K: kidney, I: iliopsoas)
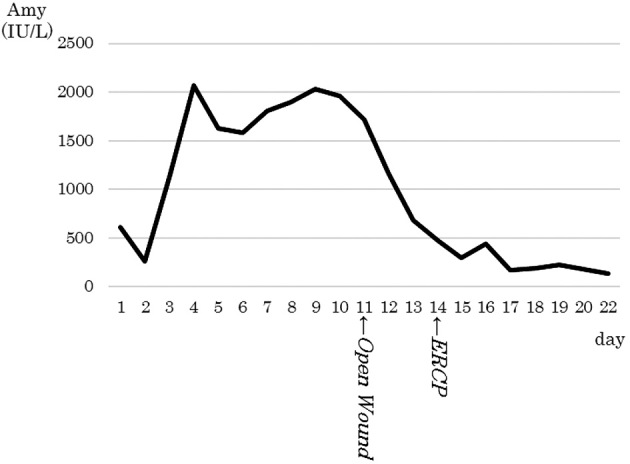
The time course of the serum amylase level. The serum amylase level increased after admission due to the worsening of the patient’s pancreatitis, and decreased after the opening of the incised wound in the femoral region.
Similar articles
-
Hepatobiliary and Pancreatic: Intraductal papillary mucinous neoplasm rupture: A rare cause of pancreatic fistula.J Gastroenterol Hepatol. 2020 Apr;35(4):528. doi: 10.1111/jgh.14882. Epub 2019 Dec 10. J Gastroenterol Hepatol. 2020. PMID: 31822035 Review. No abstract available.
-
Malignant intraductal papillary mucinous neoplasm of the pancreas with multiple pancreatogastric fistulas: a report of 2 cases with different features.Gastrointest Endosc. 2007 Oct;66(4):854-7. doi: 10.1016/j.gie.2007.01.019. Epub 2007 Aug 24. Gastrointest Endosc. 2007. PMID: 17719044 No abstract available.
-
Biliopancreatic fistula and abscess formation in the bursa omentalis associated with intraductal papillary mucinous cancer of the pancreas.Int J Clin Oncol. 2009 Oct;14(5):460-4. doi: 10.1007/s10147-008-0864-1. Epub 2009 Oct 25. Int J Clin Oncol. 2009. PMID: 19856058
-
A case of pancreaticobiliary fistula associated with an intraductal papillary mucinous neoplasm of the pancreas.Jpn J Clin Oncol. 2015 Feb;45(2):232. doi: 10.1093/jjco/hyu217. Jpn J Clin Oncol. 2015. PMID: 25589455 No abstract available.
-
Biliopancreatic fistula associated with intraductal papillary-mucinous pancreatic cancer: institutional experience and review of the literature.Hepatogastroenterology. 2000 Jul-Aug;47(34):1164-7. Hepatogastroenterology. 2000. PMID: 11020905 Review.
Cited by
-
A Case of Pancreatic Duct Leak Presenting as Lower Extremity Pain and Edema.Cureus. 2021 Oct 17;13(10):e18839. doi: 10.7759/cureus.18839. eCollection 2021 Oct. Cureus. 2021. PMID: 34804694 Free PMC article.
-
Main-Duct Intraductal Papillary Mucinous Neoplasm Complicated by a Pancreaticogastric Fistula and a Pancreaticocholedocal Fistula.Cureus. 2023 May 3;15(5):e38502. doi: 10.7759/cureus.38502. eCollection 2023 May. Cureus. 2023. PMID: 37273307 Free PMC article.
-
A Rare Case of Intraductal Tubulopapillary Neoplasm of the Pancreas Rupturing and Causing Acute Peritonitis.Case Rep Gastroenterol. 2017 Nov 2;11(3):661-666. doi: 10.1159/000481935. eCollection 2017 Sep-Dec. Case Rep Gastroenterol. 2017. PMID: 29282388 Free PMC article.
-
Rupture of small cystic pancreatic neuroendocrine tumor with many microtumors.World J Gastroenterol. 2017 Oct 7;23(37):6911-6919. doi: 10.3748/wjg.v23.i37.6911. World J Gastroenterol. 2017. PMID: 29085235 Free PMC article.
References
-
- Semba D, Wada Y, Ishihara Y, Kaji T, Kuroda A, Morioka Y. Massive pancreatic pleural effusion: pathogenesis of pancreatic duct disruption. Gastroenterol 99: 528-532, 1990. - PubMed
-
- Takahashi S, Homma H, Akiyama T, et al. . A case of intraductal papillary mucinous neoplasm with internal pancreatic fistula causing left ureteral obstruction. Jpn J Gastroenterol 104: 1236-1244, 2007. (in Japanese, Abstract in English). - PubMed
-
- Kuroda A, Semba D, Nagai H, Atomi Y, Morioka Y. Pancreatic pleural effusions and ascites. Tan to Sui 7: 407-415, 1986(in Japanese).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical