

Portal vein embolization for induction of selective hepatic hypertrophy prior to major hepatectomy: rationale, techniques, outcomes and future directions
- PMID: 28154774
- PMCID: PMC5250600
- DOI: 10.20892/j.issn.2095-3941.2016.0083
Portal vein embolization for induction of selective hepatic hypertrophy prior to major hepatectomy: rationale, techniques, outcomes and future directions
Abstract
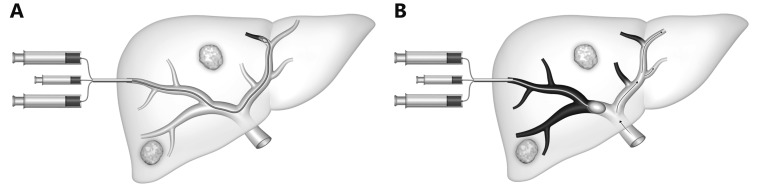
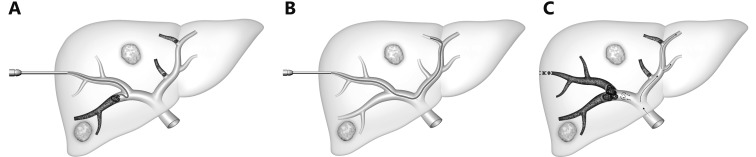
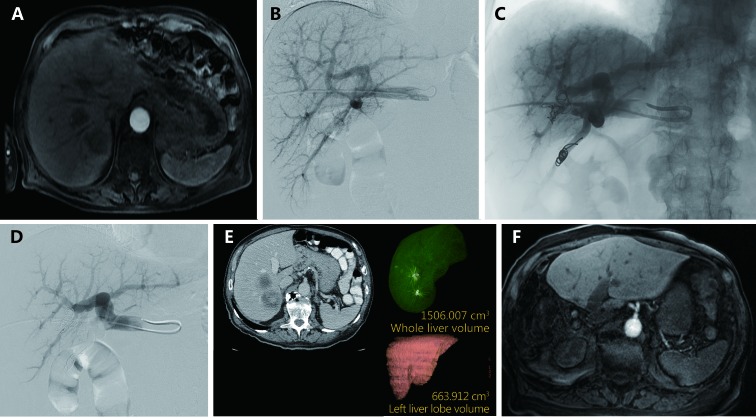
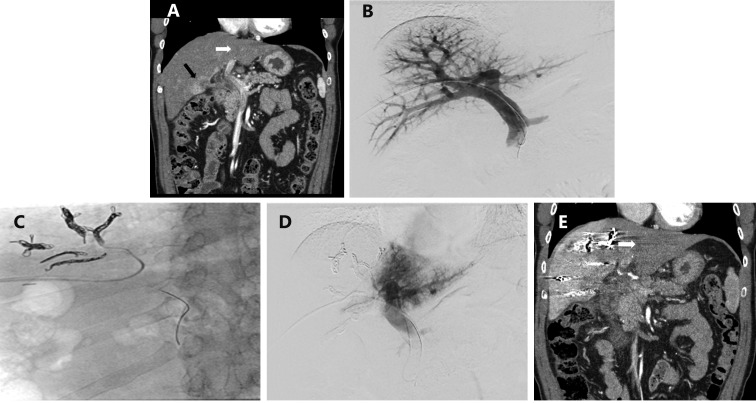
The ability to modulate the future liver remnant (FLR) is a key component of modern oncologic hepatobiliary surgery practice and has extended surgical candidacy for patients who may have been previously thought unable to survive liver resection. Multiple techniques have been developed to augment the FLR including portal vein embolization (PVE), associating liver partition and portal vein ligation (ALPPS), and the recently reported transhepatic liver venous deprivation (LVD). PVE is a well-established means to improve the safety of liver resection by redirecting blood flow to the FLR in an effort to selectively hypertrophy and ultimately improve functional reserve of the FLR. This article discusses the current practice of PVE with focus on summarizing the large number of published reports from which outcomes based practices have been developed. Both technical aspects of PVE including volumetry, approaches, and embolization agents; and clinical aspects of PVE including data supporting indications, and its role in conjunction with chemotherapy and transarterial embolization will be highlighted. PVE remains an important aspect of oncologic care; in large part due to the substantial foundation of information available demonstrating its clear clinical benefit for hepatic resection candidates with small anticipated FLRs.
Keywords: Portal vein; embolization; future liver remnant; hepatocellular carcinoma; hypertrophy; liver cancer; liver metastases; liver regeneration.
Figures
References
-
- Tjandra JJ, Fan ST, Wong J. Peri-operative mortality in hepatic resection. Aust N Z J Surg. 1991;61:201–6. - PubMed
-
- Shirabe K, Shimada M, Gion T, Hasegawa H, Takenaka K, Utsunomiya T, et al. Postoperative liver failure after major hepatic resection for hepatocellular carcinoma in the modern era with special reference to remnant liver volume. J Am Coll Surg. 1999;188:304–9. - PubMed
-
- Aloia TA. Associating liver partition and portal vein ligation for staged hepatectomy: portal vein embolization should remain the gold standard. JAMA Surg. 2015;150:927–8. - PubMed
-
- Guiu B, Chevallier P, Denys A, Delhom E, Pierredon-Foulongne MA, Rouanet P, et al. Simultaneous trans-hepatic portal and hepatic vein embolization before major hepatectomy: the liver venous deprivation technique. Eur Radiol. 2016;26:4259–67. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources