

Comparative performance of non-contrast MRI with HASTE vs. contrast-enhanced MRI/3D-MRCP for possible choledocholithiasis in hospitalized patients
- PMID: 28154911
- PMCID: PMC5457321
- DOI: 10.1007/s00261-016-1039-6
Comparative performance of non-contrast MRI with HASTE vs. contrast-enhanced MRI/3D-MRCP for possible choledocholithiasis in hospitalized patients
Abstract
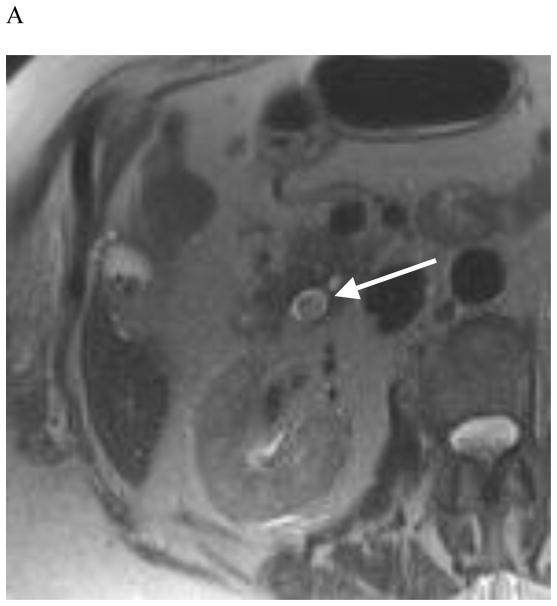
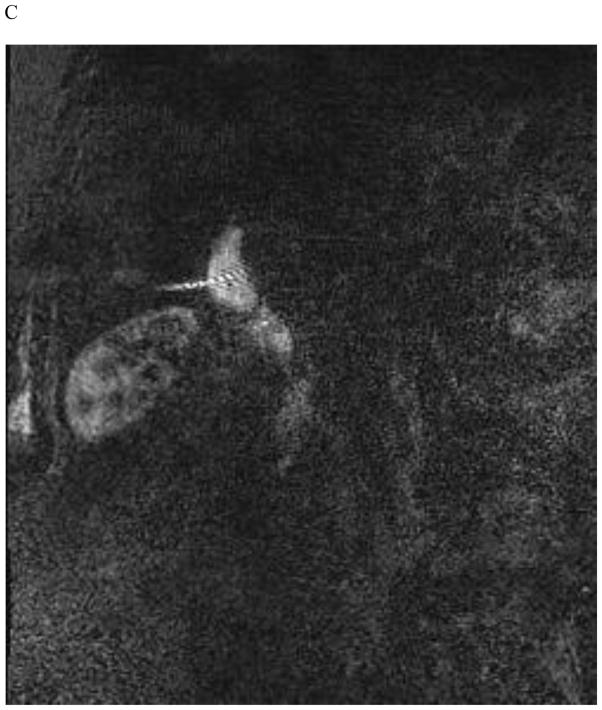
Purpose: To compare the performance of non-contrast MRI with half-Fourier acquisition single-shot turbo spin echo (HASTE) vs. contrast-enhanced MRI/3D-MRCP for assessment of suspected choledocholithiasis in hospitalized patients.
Methods and materials: 123 contrast-enhanced abdominal MRI/MRCP scans in the hospital setting for possible choledocholithiasis were retrospectively evaluated. Endoscopic retrograde cholangiopancreatography, intraoperative cholangiogram or documented clinical resolution served as the reference standard. Readers first evaluated the biliary tree using coronal and axial HASTE and other non-contrast sequences, and later reviewed the entire exam with post-contrast sequences and 3D-MRCP. Test performance for the image sets was compared for choledocholithiasis, acute hepatitis, cholangitis, and acute cholecystitis. Reader agreement, MRCP image quality, and confidence levels were also assessed. Clinical predictors of age and fever were tested for association with perceived need for contrast in biliary assessment.
Results: There were 27 cases of choledocholithiasis, 31 cases of acute hepatitis, 37 cases of acute cholecystitis, and 3 clinically diagnosed cases of acute cholangitis. Both the abbreviated and full contrast-enhanced/MRCP image sets resulted in high accuracy for choledocholithiasis (91.1-94.3% vs. 91.9-92.7%). There was no difference in sensitivity or specificity for either reader for any diagnosis between image sets (p > 0.40). 1 reader showed improved confidence (p < 0.001) with inclusion of MRCP and contrast-enhanced images, but neither confidence nor MRCP quality scores were associated with diagnostic accuracy. Patient age and fever did not predict the need for contrast-enhanced images.
Conclusion: In hospitalized patients with suspected choledocholithiasis, performance of non-contrast abdominal MRI with HASTE is similar to contrast-enhanced MRI with 3D-MRCP, offering potential for decreased scanning time and improved patient tolerability.
Keywords: Choledocholithiasis; Gallstone disease; HASTE; Magnetic resonance cholangiopancreatography.
Conflict of interest statement
Dr. Heacock declares that she has no conflict of interest. Drs. Doshi, Sun, Ream, and Babb declare no conflict of interest.
Figures







Similar articles
-
ACCURACY OF ABBREVIATED PROTOCOL OF MAGNETIC RESONANCE CHOLANGIO-PANCREATOGRAPHY IN THE DIAGNOSIS OF CHOLEDOCHOLITHIASIS.Arq Gastroenterol. 2022 Apr-Jun;59(2):188-192. doi: 10.1590/S0004-2803.202202000-35. Arq Gastroenterol. 2022. PMID: 35830027
-
Is MRCP necessary to diagnose pancreas divisum?BMC Med Imaging. 2019 Apr 29;19(1):33. doi: 10.1186/s12880-019-0329-1. BMC Med Imaging. 2019. PMID: 31035952 Free PMC article.
-
Accuracy and timeliness of an abbreviated emergency department MRCP protocol for choledocholithiasis.Emerg Radiol. 2019 Aug;26(4):427-432. doi: 10.1007/s10140-019-01689-w. Epub 2019 Apr 27. Emerg Radiol. 2019. PMID: 31030393
-
Utility of MRCP in clinical decision making of suspected choledocholithiasis: An institutional analysis and literature review.Am J Surg. 2017 Aug;214(2):251-255. doi: 10.1016/j.amjsurg.2016.10.025. Epub 2016 Dec 1. Am J Surg. 2017. PMID: 27986260 Review.
-
Diagnostic accuracy of EUS compared with MRCP in detecting choledocholithiasis: a meta-analysis of diagnostic test accuracy in head-to-head studies.Gastrointest Endosc. 2017 Dec;86(6):986-993. doi: 10.1016/j.gie.2017.06.009. Epub 2017 Jun 20. Gastrointest Endosc. 2017. PMID: 28645544 Review.
Cited by
-
Influence of Percutaneous Drainage Surgery and the Interval to Perform Laparoscopic Cholecystectomy on Acute Cholecystitis through Genetic Algorithm-Based Contrast-Enhanced Ultrasound Imaging.Comput Intell Neurosci. 2022 Jul 30;2022:3602811. doi: 10.1155/2022/3602811. eCollection 2022. Comput Intell Neurosci. 2022. PMID: 35942459 Free PMC article.
-
A Case of Hemorrhagic Cholecystitis in a Patient on Apixaban After COVID-19 Infection.Am J Case Rep. 2023 Jul 21;24:e939677. doi: 10.12659/AJCR.939677. Am J Case Rep. 2023. PMID: 37475204 Free PMC article.
-
Improving MR sequence of 18F-FDG PET/MR for diagnosing and staging gastric Cancer: a comparison study to 18F-FDG PET/CT.Cancer Imaging. 2020 Jun 16;20(1):39. doi: 10.1186/s40644-020-00317-y. Cancer Imaging. 2020. PMID: 32546207 Free PMC article.
-
Traveling gallstones: review of MR imaging and surgical pathology features of gallstone disease and its complications in the gallbladder and beyond.Abdom Radiol (NY). 2024 Mar;49(3):722-737. doi: 10.1007/s00261-023-04107-5. Epub 2023 Dec 3. Abdom Radiol (NY). 2024. PMID: 38044336 Review.
-
Decreasing inappropriate MRCP with contrast exams: impact of an EMR-Embedded clinical care pathway.Abdom Radiol (NY). 2025 May 29. doi: 10.1007/s00261-025-05022-7. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40439723
References
-
- Committee ASoP. Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, et al. The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointestinal endoscopy. 2010;71(1):1–9. - PubMed
-
- Shaffer EA. Epidemiology and risk factors for gallstone disease: has the paradigm changed in the 21st century? Current gastroenterology reports. 2005;7(2):132–40. - PubMed
-
- Topal B, Van de Moortel M, Fieuws S, Vanbeckevoort D, Van Steenbergen W, Aerts R, et al. The value of magnetic resonance cholangiopancreatography in predicting common bile duct stones in patients with gallstone disease. The British journal of surgery. 2003;90(1):42–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
