

Critical Thinking in Critical Care: Five Strategies to Improve Teaching and Learning in the Intensive Care Unit
- PMID: 28157389
- PMCID: PMC5461985
- DOI: 10.1513/AnnalsATS.201612-1009AS
Critical Thinking in Critical Care: Five Strategies to Improve Teaching and Learning in the Intensive Care Unit
Abstract
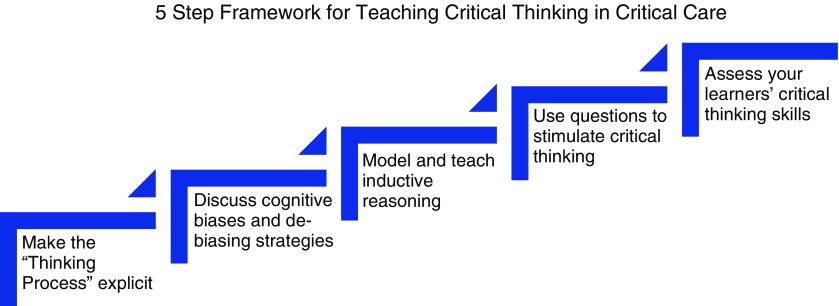
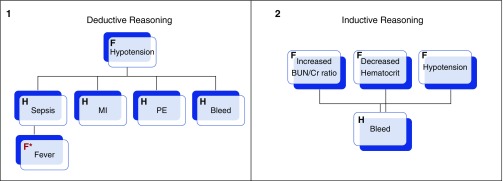
Critical thinking, the capacity to be deliberate about thinking, is increasingly the focus of undergraduate medical education, but is not commonly addressed in graduate medical education. Without critical thinking, physicians, and particularly residents, are prone to cognitive errors, which can lead to diagnostic errors, especially in a high-stakes environment such as the intensive care unit. Although challenging, critical thinking skills can be taught. At this time, there is a paucity of data to support an educational gold standard for teaching critical thinking, but we believe that five strategies, routed in cognitive theory and our personal teaching experiences, provide an effective framework to teach critical thinking in the intensive care unit. The five strategies are: make the thinking process explicit by helping learners understand that the brain uses two cognitive processes: type 1, an intuitive pattern-recognizing process, and type 2, an analytic process; discuss cognitive biases, such as premature closure, and teach residents to minimize biases by expressing uncertainty and keeping differentials broad; model and teach inductive reasoning by utilizing concept and mechanism maps and explicitly teach how this reasoning differs from the more commonly used hypothetico-deductive reasoning; use questions to stimulate critical thinking: "how" or "why" questions can be used to coach trainees and to uncover their thought processes; and assess and provide feedback on learner's critical thinking. We believe these five strategies provide practical approaches for teaching critical thinking in the intensive care unit.
Keywords: cognitive errors; critical care; critical thinking; medical education.
Figures
Comment in
-
Teaching: A Newer Face.Air Med J. 2017 Nov-Dec;36(6):282-286. doi: 10.1016/j.amj.2017.09.006. Air Med J. 2017. PMID: 29132587 No abstract available.
References
-
- Scriven M, Paul R. Critical thinking as defined by the national council for excellence in critical thinking. Presented at the 8th Annual International Conference on Critical Thinking and Education Reform; August 1987; Rohnert Park, California.
-
- Huang GC, Newman LR, Schwartzstein RM. Critical thinking in health professions education: summary and consensus statements of the Millennium Conference 2011. Teach Learn Med. 2014;26:95–102. - PubMed
-
- Croskerry P. From mindless to mindful practice--cognitive bias and clinical decision making. N Engl J Med. 2013;368:2445–2448. - PubMed
-
- Facione P. Critical thinking: What it is and why it counts. Millbrae, CA: The California Academic Press; 2011.
-
- Tversky A, Kahneman D. Judgement under uncertainty: heuristics and biases. Science. 1974;185:1124–1131. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
