

Factors Determining In Vitro Lung Deposition of Albuterol Aerosol Delivered by Ventolin Metered-Dose Inhaler
- PMID: 28157430
- PMCID: PMC5564031
- DOI: 10.1089/jamp.2015.1278
Factors Determining In Vitro Lung Deposition of Albuterol Aerosol Delivered by Ventolin Metered-Dose Inhaler
Abstract
Background: The effectiveness of metered-dose inhalers (MDIs) in delivering medication to the lungs highly depends on its correct usage technique. Current guidelines state optimal technique for high lung deposition should include a slow inhalation (>5 seconds) at an inspiratory flow rate of 30 L/min and inhaler actuation at the start of inhalation. However, these recommendations were based on clinical studies using CFC (chlorofluorocarbon)-MDIs and in vitro studies of HFA (hydrofluoroalkane)-MDIs using idealized MDI techniques of uniform inhalation and actuation, disregarding the nonuniform techniques of actual patients.
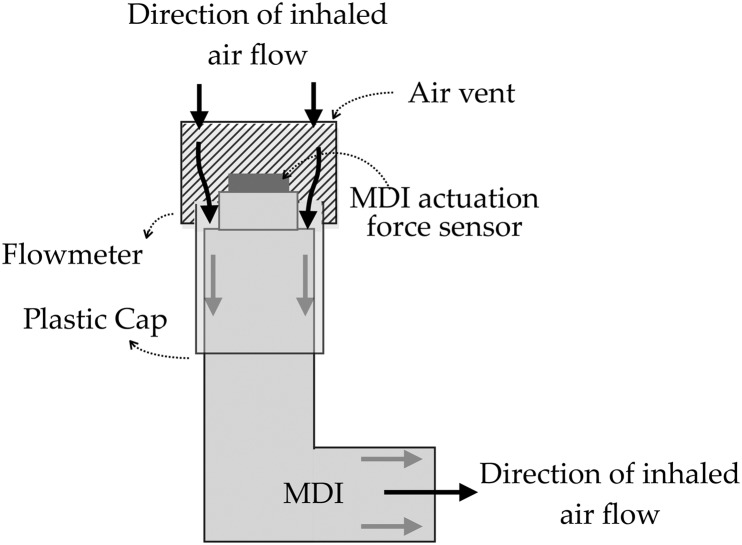
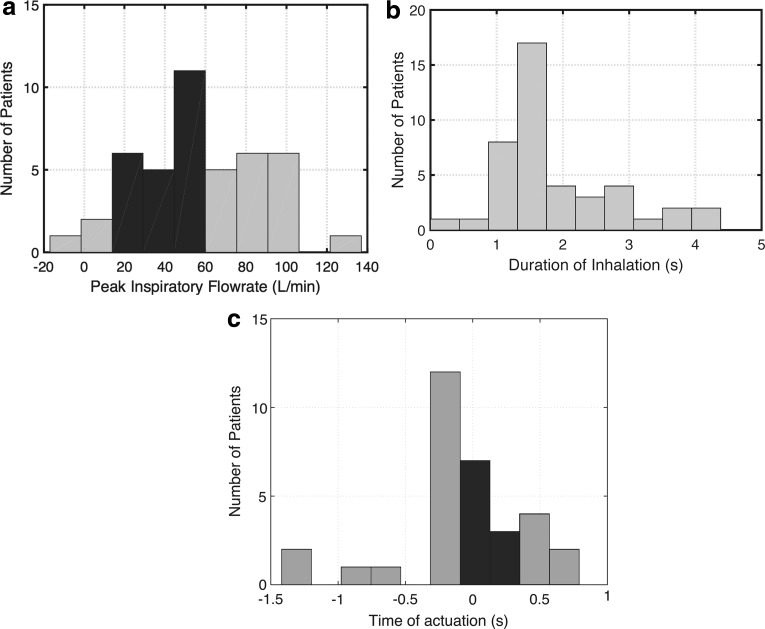
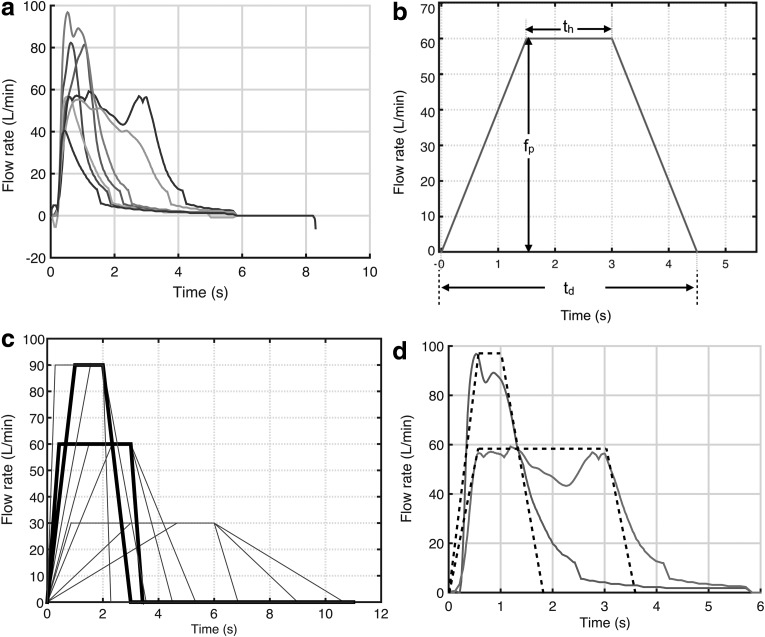
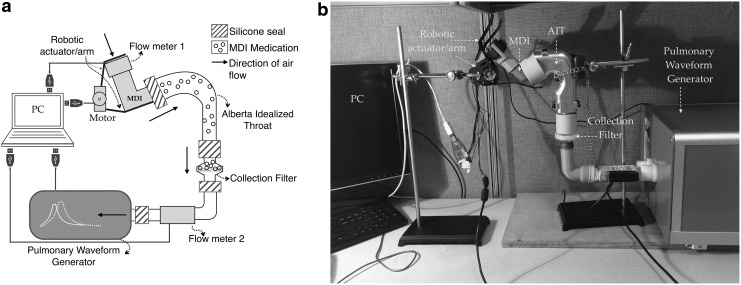
Methods: To better understand the effects of time-varying MDI usage parameters on lung deposition of aerosol delivered by an HFA-MDI, we conducted an in vitro study modeled on real-life variable inspiratory flow and actuation techniques recorded from 15 subjects with asthma/chronic obstructive pulmonary disease (COPD). We developed a model representing the time-varying inspiratory flow waveforms and actuation timings based on 43 MDI techniques recorded from patients. Furthermore, we constructed an in vitro experimental setup using a mouth-throat cast, programmable MDI actuator, and breath simulator to evaluate lung deposition for the MDI techniques derived from our model.
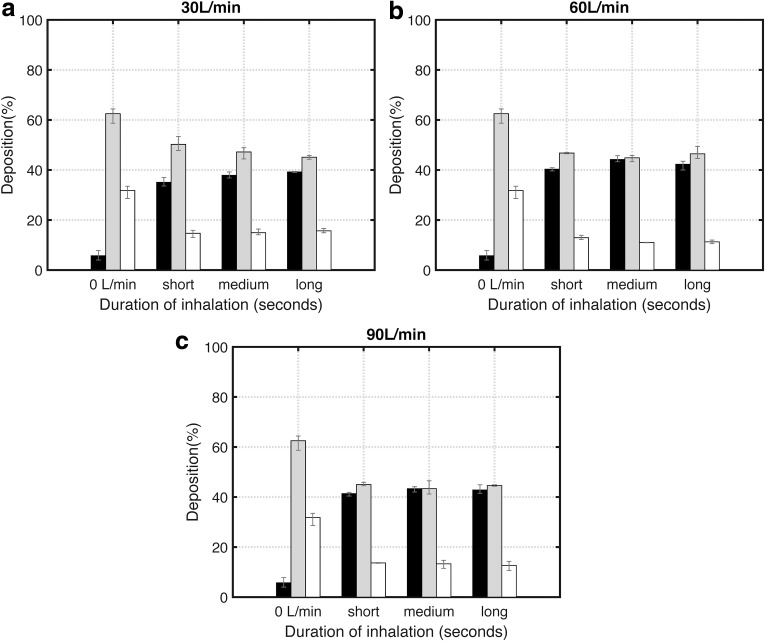
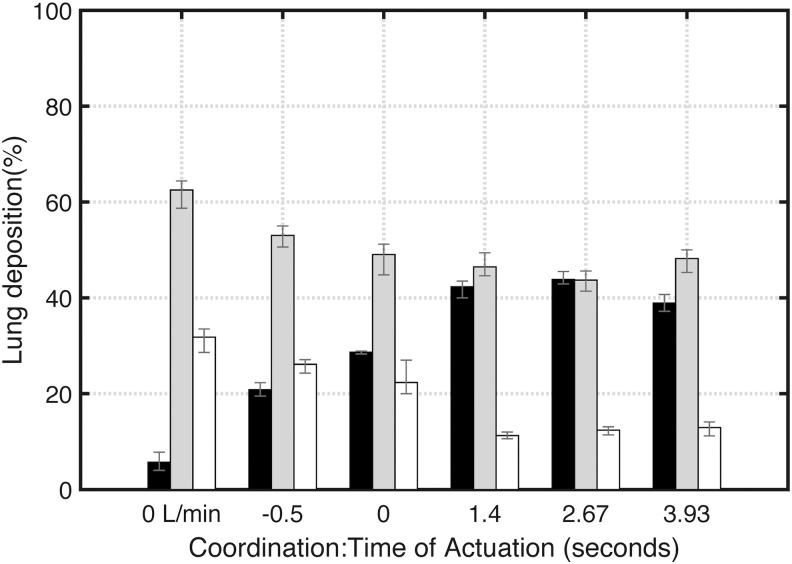
Results: High inspiratory flow rates, 60-90 L/min, consistently resulted in high in vitro lung deposition (>40%) of aerosol (albuterol delivered from Ventolin HFA-MDI) compared to 30 L/min when MDI actuation occurred in the first half of inhalation. Also, positive coordination resulted in higher in vitro lung deposition compared with negative or zero coordination (actuating before or at the start of inspiration). Furthermore, variation in coordination affected lung deposition more significantly (23%) than flow rate or duration of inspiration (≤5%).
Conclusions: In an in vitro experimental model based on inhalation data from patients with asthma and COPD, we demonstrated that aerosol lung deposition emitted from Ventolin HFA-MDI is most optimal for MDI actuation in the first half of inspiration at high flow rates (60-90 L/min).
Keywords: COPD; aerosol; asthma; inhaler technique; lung deposition; metered-dose inhaler.
Conflict of interest statement
Dr. Ashutosh Sabharwal is a Professor, Department of Electrical and Computer Engineering at Rice University, Houston, Texas. He is also a cofounder of Cognita Labs LLC. Ms. Rajoshi Biswas is a PhD candidate in the Department of Electrical and Computer Engineering at Rice University. She is also an employee of Cognita Labs LLC. Dr. Nicola Hanania is an Associate Professor, Baylor College of Medicine; Director, Airways Clinical Research Center, Houston, Texas. No competing financial interests exist.
Figures
Similar articles
-
In vitro tests for aerosol deposition. III: effect of inhaler insertion angle on aerosol deposition.J Aerosol Med Pulm Drug Deliv. 2013 Jun;26(3):145-56. doi: 10.1089/jamp.2012.0989. Epub 2012 Oct 1. J Aerosol Med Pulm Drug Deliv. 2013. PMID: 23025452
-
Prospective, open-label assessment of albuterol sulfate hydrofluoroalkane metered-dose inhaler with new integrated dose counter.Allergy Asthma Proc. 2013 Jan-Feb;34(1):42-51. doi: 10.2500/aap.2012.33.3647. Epub 2012 Dec 20. Allergy Asthma Proc. 2013. PMID: 23265285 Clinical Trial.
-
Influence of particle size and patient dosing technique on lung deposition of HFA-beclomethasone from a metered dose inhaler.J Aerosol Med. 2005 Winter;18(4):379-85. doi: 10.1089/jam.2005.18.379. J Aerosol Med. 2005. PMID: 16379614 Clinical Trial.
-
Practical problems with aerosol therapy in COPD.Respir Care. 2006 Feb;51(2):158-72. Respir Care. 2006. PMID: 16441960 Review.
-
Inhaled corticosteroid delivery systems: clinical role of a breath-actuated device.Eur Rev Med Pharmacol Sci. 2001 Jan-Feb;5(1):7-16. Eur Rev Med Pharmacol Sci. 2001. PMID: 11860222 Review.
Cited by
-
ATTACHED, DETACHED and WITHOUT inhaler technique coaching tools to optimize pMDI use competence, asthma control and quality-of-life in asthmatic adults.J Thorac Dis. 2020 May;12(5):2415-2425. doi: 10.21037/jtd.2020.03.50. J Thorac Dis. 2020. PMID: 32642147 Free PMC article.
-
Characterization and comparison of Re-Du-Ning aerosol particles generated by different jet nebulizers.RSC Adv. 2019 Sep 25;9(52):30292-30301. doi: 10.1039/c9ra06177k. eCollection 2019 Sep 23. RSC Adv. 2019. PMID: 35530199 Free PMC article.
-
Lower Inspiratory Breathing Depth Enhances Pulmonary Delivery Efficiency of ProAir Sprays.Pharmaceuticals (Basel). 2022 Jun 3;15(6):706. doi: 10.3390/ph15060706. Pharmaceuticals (Basel). 2022. PMID: 35745624 Free PMC article.
References
-
- Capstick TG, and Clifton IJ: Inhaler technique and training in people with chronic obstructive pulmonary disease and asthma. Expert Rev Respir Med. 2012;6:91–103 - PubMed
-
- Rubin BK: What does it mean when a patient says, “My asthma medication is not working?” Chest. 2004;126:972–981 - PubMed
-
- Roche N, Chrystyn H, Lavorini F, and Agusti A: Effectiveness of inhaler devices in adult asthma and COPD. EMJ Respir. 2013;1:64–71
-
- Melani AS, Bonavia M, Cilenti V, Cinti C, Lodi M, Martucci P, Serra M, Scichilone N, Sestini P, Aliani M, and Neri M: Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105:930–938 - PubMed
-
- Laube BL, Janssens HM, De Jongh FHC, Devadason SG, Dhand R, Diot P, Everard ML, Horvath I, Navalesi P, Voshaar T, and Chrystyn H: What the pulmonary specialist should know about the new inhalation therapies. Eur Respir J. 2011;37:1308–1331 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
