

Prevalence and risk factors of taste and smell impairment in a nationwide representative sample of the US population: a cross-sectional study
- PMID: 28157672
- PMCID: PMC5129069
- DOI: 10.1136/bmjopen-2016-013246
Prevalence and risk factors of taste and smell impairment in a nationwide representative sample of the US population: a cross-sectional study
Abstract
Objectives: To estimate the prevalence of, and explore potential risk factors for, taste and smell dysfunction in the general population of the USA.
Design: A cross-sectional study.
Setting: A cross-sectional analysis of data collected in the National Health and Nutrition Examination Survey (NHANES 2013-2014).
Participants: A total of 3519 men and women aged 40 years and older who participated in NHANES 2013-2014.
Main outcome measures: Using the NHANES Pocket Smell Test, smell impairment was defined as failing to correctly identify 6 or more of the 8 odours. Taste impairment was defined as failing to correctly identify quinine or sodium chloride.
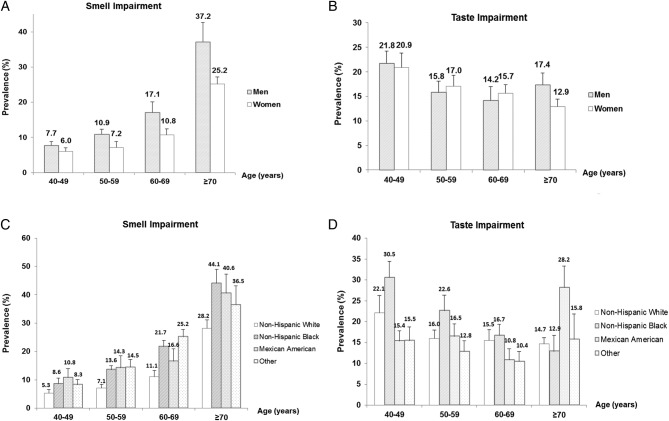
Results: The estimated prevalence was 13.5% for smell impairment, 17.3% for taste impairment and 2.2% for taste and smell impairment. For smell, but not taste, prevalence estimates increased with age and were higher in men and ethnic minorities. In backward stepwise logistic regression, low educational attainment, low family income and a history of asthma or cancer were independently associated with a higher prevalence of smell impairment, whereas light-to-moderate alcohol consumption (1-3 drinks/day) was associated with a lower prevalence of this condition. After multivariate adjustment, being non-Hispanic Black Americans, consuming ≥4 drinks of alcohol per day and having a history of cardiovascular disease (CVD) were independently associated with a higher prevalence of taste impairment.
Conclusions: Based on a nationally representative multistage probability survey among the US population aged 40 years and older, smell and taste dysfunction affected ∼20.5 million (13.5%) and 26.3 million (17.3%) individuals, respectively. Age, gender, ethnicity, educational attainment, family income, light-to-moderate alcohol consumption and history of asthma or cancer were significant risk factors for smell dysfunction, whereas only ethnicity, heavy alcohol consumption and CVD history were associated with a higher prevalence of taste dysfunction.
Keywords: Prevalence; Risk factors; Smell Impairment; Taste Impairment.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
RLD is the president and major shareholder of Sensonics International, the manufacturer of the NHANES Pocket Smell Test.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical