

Systematic lymphadenectomy versus sampling of ipsilateral mediastinal lymph-nodes during lobectomy for non-small-cell lung cancer: a systematic review of randomized trials and a meta-analysis
- PMID: 28158453
- PMCID: PMC6095012
- DOI: 10.1093/ejcts/ezw439
Systematic lymphadenectomy versus sampling of ipsilateral mediastinal lymph-nodes during lobectomy for non-small-cell lung cancer: a systematic review of randomized trials and a meta-analysis
Erratum in
-
Corrigendum to 'Systematic lymphadenectomy versus sampling of ipsilateral mediastinal lymph-nodes during lobectomy for non-small cell lung cancer: a systematic review of randomized trials and a meta-analysis' [Eur J Cardiothorac Surg 2017;51:1149-1156].Eur J Cardiothorac Surg. 2018 Oct 1;54(4):795. doi: 10.1093/ejcts/ezy297. Eur J Cardiothorac Surg. 2018. PMID: 30124846 Free PMC article. No abstract available.
Abstract
Objectives: To re-examine the evidence for recommendations for complete dissection versus sampling of ipsilateral mediastinal lymph nodes during lobectomy for cancer.
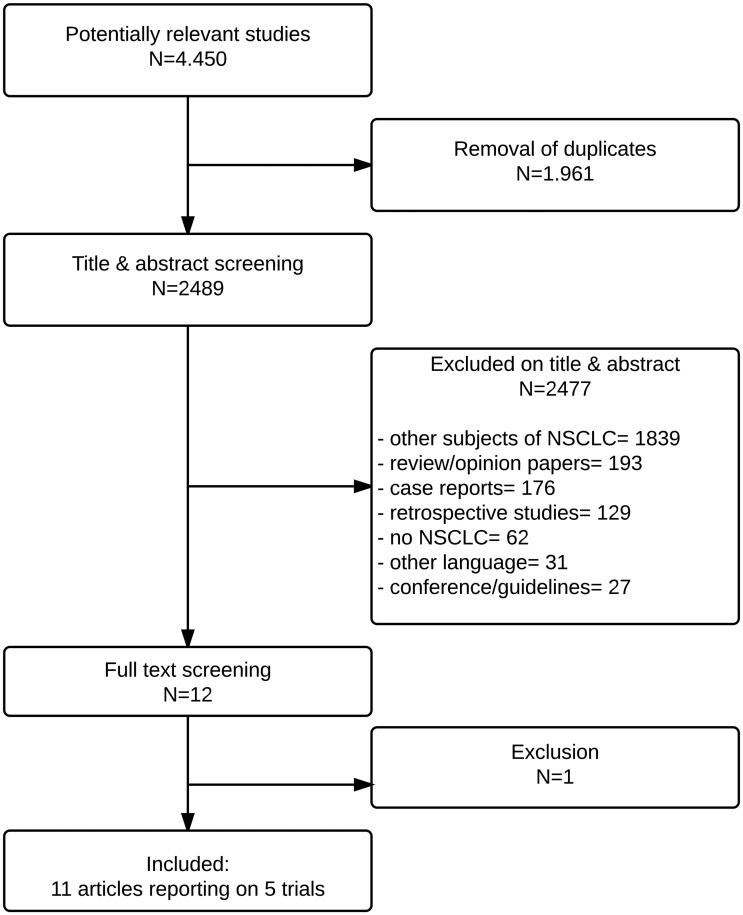
Methods: We searched for randomized trials of systematic mediastinal lymphadenectomy versus mediastinal sampling. We performed a textual analysis of the authors' own starting assumptions and conclusion. We analysed the trial designs and risk of bias. We extracted data on early mortality, perioperative complications, overall survival, local recurrence and distant recurrence for meta-analysis.
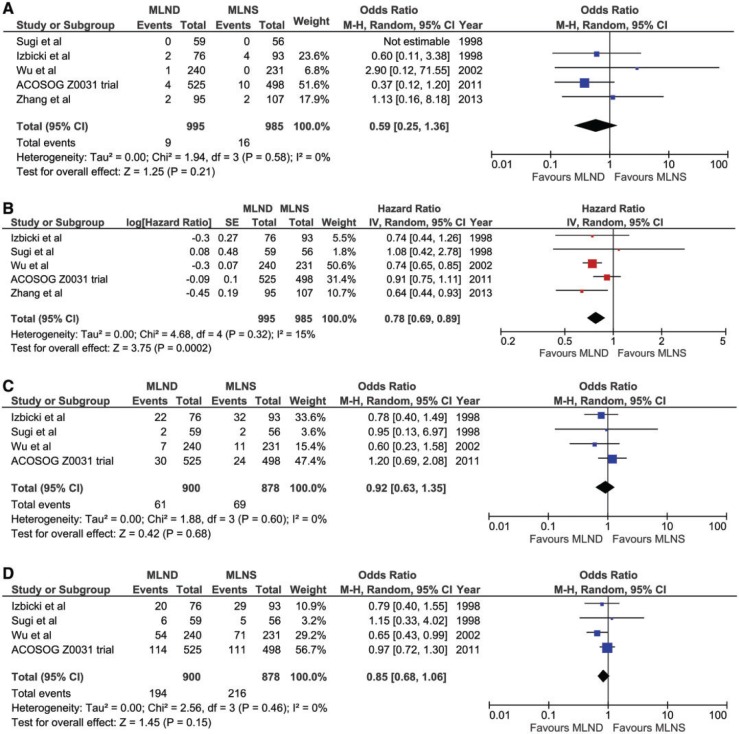
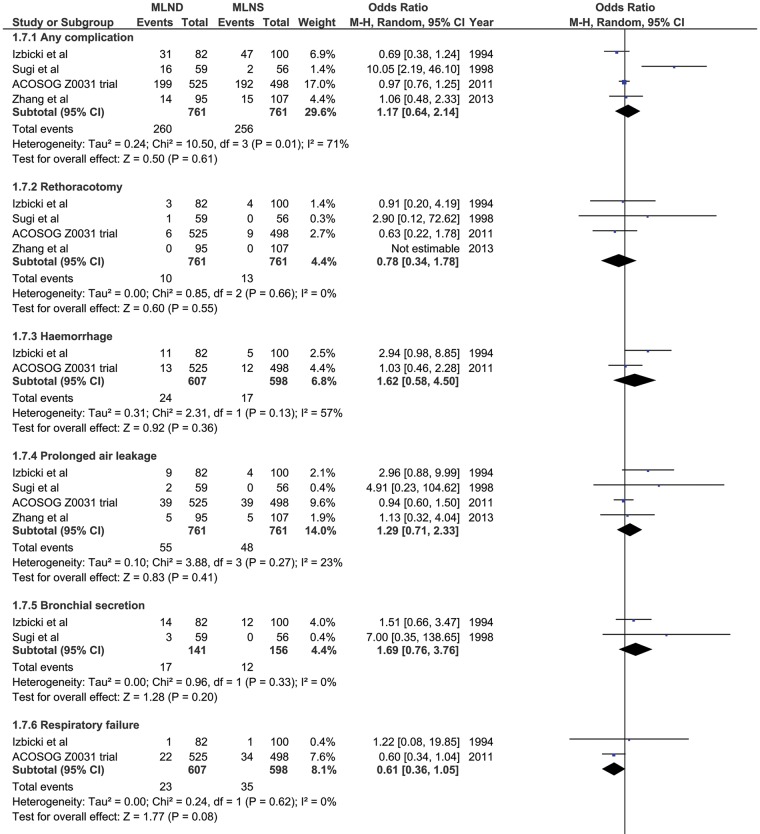
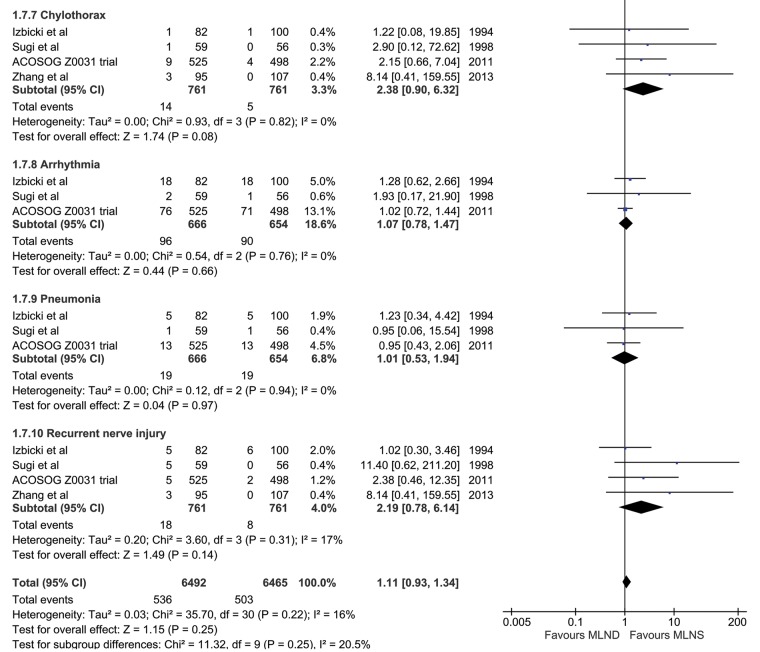
Results: We found five randomized controlled trials recruiting 1980 patients spanning 1989-2007. The expressed starting position in 3/5 studies was a conviction that systematic dissection was effective. Long-term survival was better with lymphadenectomy compared with sampling (Hazard Ratio 0.78; 95% CI 0.69-0.89) as was perioperative survival (Odds Ratio 0.59; 95% CI 0.25-1.36, non-significant). But there was an overall high risk of bias and a lack of intention to treat analysis. There were higher rates (non-significant) of perioperative complications including bleeding, chylothorax and recurrent nerve palsy with lymphadenectomy.
Conclusions: The high risk of bias in these trials makes the overall conclusion insecure. The finding of clinically important surgically related morbidities but lower perioperative mortality with lymphadenectomy seems inconsistent. The multiple variables in patients, cancers and available treatments suggest that large pragmatic multicentre trials, testing currently available strategies, are the best way to find out which are more effective. The number of patients affected with lung cancer makes trials feasible.
Keywords: Lung cancer; Lymph node staging; Surgery.
© The Author 2017. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures
Comment in
-
Systematic lymphadenectomy: 'meta-lysis' does not need meta-analysis.Eur J Cardiothorac Surg. 2017 Nov 1;52(5):1011-1012. doi: 10.1093/ejcts/ezx299. Eur J Cardiothorac Surg. 2017. PMID: 28950369 No abstract available.
-
Reply to Riquet.Eur J Cardiothorac Surg. 2017 Nov 1;52(5):1012-1013. doi: 10.1093/ejcts/ezx300. Eur J Cardiothorac Surg. 2017. PMID: 28950370 No abstract available.
-
Complete mediastinal lymph node dissection versus systematic lymph node sampling in surgical treatment of non-small cell lung cancer: do we have the answer?J Thorac Dis. 2017 Nov;9(11):4169-4170. doi: 10.21037/jtd.2017.10.39. J Thorac Dis. 2017. PMID: 29268461 Free PMC article. No abstract available.
References
-
- Lardinois D, De Leyn P, van Schil P, Porta RR, Waller D, Passlick B, et al. ESTS guidelines for intraoperative lymph node staging in non-small cell lung cancer. Eur J Cardiothorac Surg 2006;30:787–92. - PubMed
-
- Asamura H, Chansky K, Crowley J, Goldstraw P, Rusch VW, Vansteenkiste JF, et al. The International association for the study of lung cancer lung cancer staging project: proposals for the revision of the n descriptors in the forthcoming 8th edition of the tnm classification for lung cancer. J Thorac Oncol 2015;10:1675–84. - PubMed
-
- Navani N, Nankivell M, Lawrence DR, Lock S, Makker H, Baldwin DR, et al. Lung cancer diagnosis and staging with endobronchial ultrasound-guided transbronchial needle aspiration compared with conventional approaches: an open-label, pragmatic, randomised controlled trial. Lancet Respir Med 2015;3:282–89. - PMC - PubMed
-
- Slavova-Azmanova NS, Lizama C, Johnson CE, Ludewick HP, Lester L, Karunarathne S, et al. Impact of the introduction of EBUS on time to management decision, complications, and invasive modalities used to diagnose and stage lung cancer: a pragmatic pre-post study. BMC Cancer 2016. 28;16:44. - PMC - PubMed
-
- Lim E, McElnay PJ, Rocco G, Brunelli A, Massard G, Toker A, et al. Invasive mediastinal staging is irrelevant for PET/CT positive N2 lung cancer if the primary tumour and ipsilateral lymph nodes are resectable. Lancet Respir Med 2015;3:e32–e33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
