

The association between physical activity and risk of mortality is modulated by grip strength and cardiorespiratory fitness: evidence from 498 135 UK-Biobank participants
- PMID: 28158566
- PMCID: PMC5837781
- DOI: 10.1093/eurheartj/ehw249
The association between physical activity and risk of mortality is modulated by grip strength and cardiorespiratory fitness: evidence from 498 135 UK-Biobank participants
Abstract
Aims: It is unclear whether the potential benefits of physical activity differ according to level of cardiorespiratory fitness (CRF) or strength. The aim of this study was to determine whether the association between physical activity and mortality is moderated by CRF and grip strength sufficiently to inform health promotion strategies.
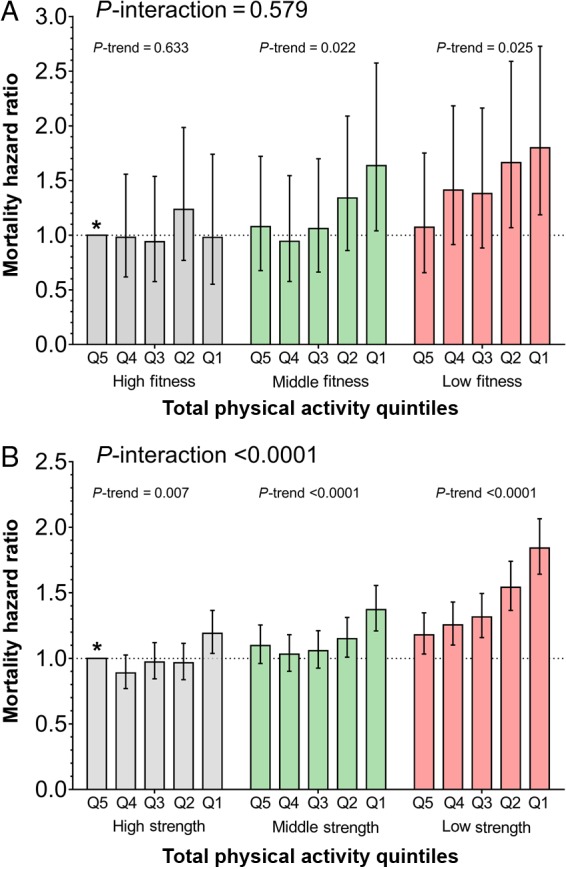
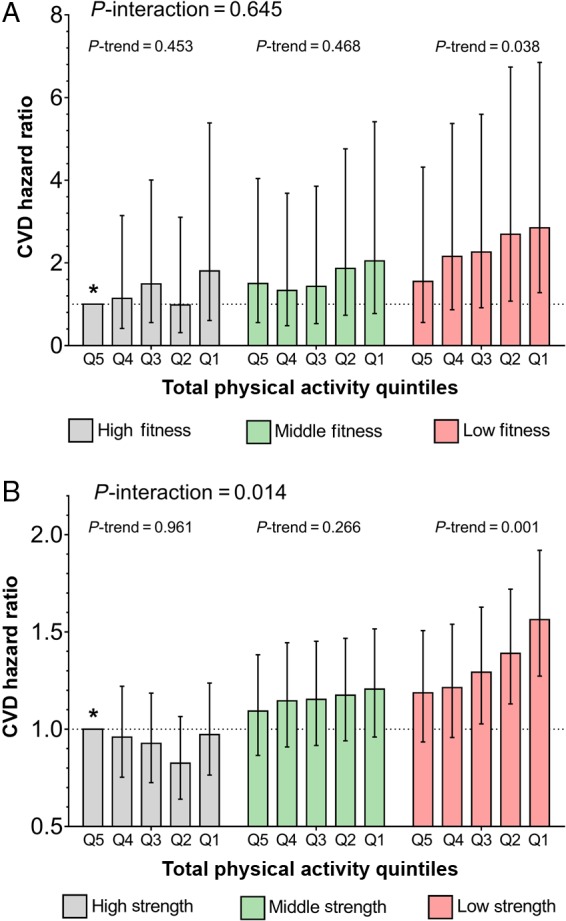
Methods and results: 498 135 participants (54.7% women) from the UK Biobank were included (CRF data available in 67 702 participants). Exposure variables were grip strength, CRF, and physical activity. All-cause mortality and cardiovascular disease (CVD) events were the outcomes. 8591 died over median 4.9 years [IQR 4.3–5.5] follow-up. There was a significant interaction between total physical activity and grip strength (P < 0.0001) whereby the higher hazard of mortality associated with lower physical activity was greatest among participants in the lowest tertile for grip strength (hazard ratio, HR:1.11 [95% CI 1.09–1.14]) and lowest among those in the highest grip strength tertile (HR:1.04 [1.01–1.08]). The interaction with CRF did not reach statistical significance but the pattern was similar. The association between physical activity and mortality was larger among those in the lowest tertile of CRF (HR:1.13 [1.02–1.26]) than those in the highest (HR:1.03 [0.91–1.16]). The pattern for CVD events was similar.
Conclusions: These data provide novel evidence that strength, and possibly CRF, moderate the association between physical activity and mortality. The association between physical activity and mortality is strongest in those with the lowest strength (which is easily measured), and the lowest CRF, suggesting that these sub-groups could benefit most from interventions to increase physical activity.
Figures
References
-
- Blair SN, Cheng Y, Holder JS. Is physical activity or physical fitness more important in defining health benefits? Med Sci Sports Exercise 2001;33:S379–S399. - PubMed
-
- Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, Sugawara A, Totsuka K, Shimano H, Ohashi Y, Yamada N, Sone H. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women a meta-analysis. J Am Med Assoc 2009;301:2024–2035. - PubMed
-
- Church TS, Earnest CP, Skinner JS, Blair SN. Effects of different doses of physical activity on cardiorespiratory fitness among sedentary, overweight or obese postmenopausal women with elevated blood pressure – a randomized controlled trial. J Am Med Assoc 2007;297:2081–2091. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
