

Early exposure to hyperoxia and mortality in critically ill patients with severe traumatic injuries
- PMID: 28158980
- PMCID: PMC5291954
- DOI: 10.1186/s12890-017-0370-1
Early exposure to hyperoxia and mortality in critically ill patients with severe traumatic injuries
Abstract
Background: Hyperoxia is common early in the course of resuscitation of critically ill patients. It has been associated with mortality in some, but not all, studies of cardiac arrest patients and other critically ill cohorts. Reasons for the inconsistency are unclear and may depend on unmeasured patient confounders, the timing and duration of hyperoxia, population characteristics, or the way that hyperoxia is defined and measured. We sought to determine whether, in a prospectively collected cohort of mechanically ventilated patients with traumatic injuries with and without head trauma, higher maximum partial pressure of arterial oxygen (PaO2) within 24 hours of admission would be associated with increased risk of in-hospital mortality.
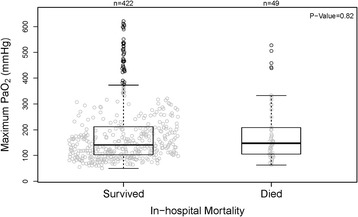
Methods: Critically ill patients with traumatic injuries undergoing invasive mechanical ventilation enrolled in the Validating Acute Lung Injury biomarkers for Diagnosis (VALID) study were included in this study. All arterial blood gases (ABGs) from the first 24 hours of admission were recorded. Primary analysis was comparison of the highest PaO2 between hospital survivors and non-survivors.
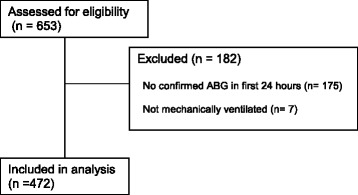
Results: A total of 653 patients were evaluated for inclusion. Of these, 182 were not mechanically ventilated or did not have an ABG measured in the first 24 hours, leaving 471 patients in the primary analysis. In survivors, the maximum PaO2 was 141 mmHg (median, interquartile range 103 - 212) compared to 148 mmHg (IQR 105 - 209) in non-survivors (p = 0.82). In the subgroup with head trauma (n = 266), the maximum PaO2 was 133 mmHg (IQR 97 - 187) among survivors and 152 mmHg (108 - 229) among nonsurvivors (p = 0.19). After controlling for age, injury severity score, number of arterial blood gases, and fraction of inspired oxygen, maximum PaO2 was not associated with increased mortality (OR 1.27 for every fold increase of PaO2 (95% CI 0.72 - 2.25).
Conclusions: In mechanically ventilated patients with severe traumatic injuries, hyperoxia in the first 24 hours of admission was not associated with increased risk of death or worsened neurological outcomes in a setting without brain tissue oxygenation monitoring.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
