

Hypertension management in rural primary care facilities in Zambia: a mixed methods study
- PMID: 28158981
- PMCID: PMC5292001
- DOI: 10.1186/s12913-017-2063-0
Hypertension management in rural primary care facilities in Zambia: a mixed methods study
Abstract
Background: Improved primary health care is needed in developing countries to effectively manage the growing burden of hypertension. Our objective was to evaluate hypertension management in Zambian rural primary care clinics using process and outcome indicators to assess the screening, monitoring, treatment and control of high blood pressure.
Methods: Better Health Outcomes through Mentoring and Assessment (BHOMA) is a 5-year, randomized stepped-wedge trial of improved clinical service delivery underway in 46 rural Zambian clinics. Clinical data were collected as part of routine patient care from an electronic medical record system, and reviewed for site performance over time according to hypertension related indicators: screening (blood pressure measurement), management (recorded diagnosis, physical exam or urinalysis), treatment (on medication), and control. Quantitative data was used to develop guides for qualitative in-depth interviews, conducted with health care providers at a proportional sample of half (20) of clinics. Qualitative data was iteratively analyzed for thematic content.
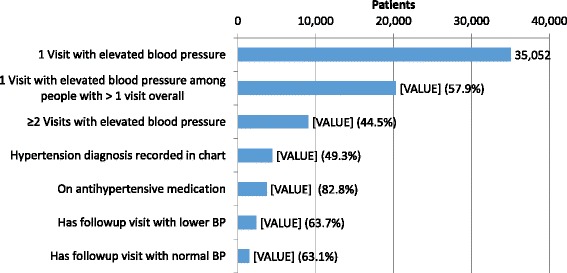
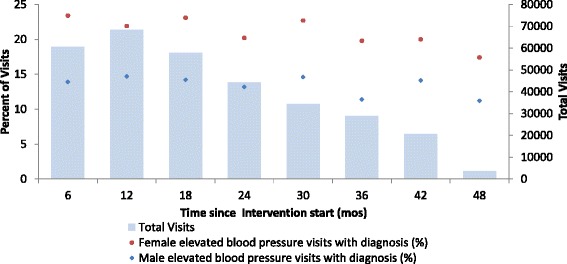
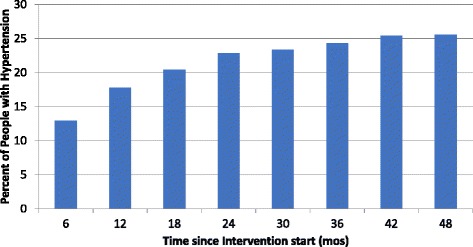
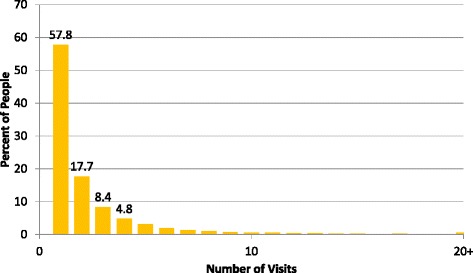
Results: From January 2011 to December 2014, 318,380 visits to 46 primary care clinics by adults aged ≥ 25 years with blood pressure measurements were included. Blood pressure measurement at vital sign screening was initially high at 89.1% overall (range: 70.1-100%), but decreased to 62.1% (range: 0-100%) by 48 months after intervention start. The majority of hypertensive patients made only one visit to the clinics (57.8%). Out of 9022 patients with at least two visits with an elevated blood pressure, only 49.3% had a chart recorded hypertension diagnosis. Process indicators for monitoring hypertension were <10% and did not improve with time. In in-depth interviews, antihypertensive medication shortages were common, with 15/20 clinics reporting hydrochlorothiazide-amiloride stockouts. Principal challenges in hypertension management included 1) equipment and personnel shortages, 2) provider belief that multiple visits were needed before official management, 3) medication stock-outs, leading to improper prescriptions and 4) poor patient visit attendance.
Conclusions: Our findings suggest that numerous barriers stand in the way of hypertension diagnosis and management in Zambian primary health facilities. Future work should focus on performance indicator development and validation in low resource contexts, to facilitate regular and systematic data review to improve patient outcomes.
Trial registration: ClinicalTrials.gov, Identifier NCT01942278 . Date of Registration: September 2013.
Keywords: Antihypertensive medication; Hypertension; Mixed methods; Performance indicators; Quality improvement; Zambia.
Figures

References
-
- Alwan A. Global status report on noncommunicable diseases 2010. Geneva: WHO; 2011.
-
- WHO Global Health Observatory. Noncommunicable Diseases [database on the Internet]. Geneva: WHO; 2012. http://www.who.int/gho/ncd. Accessed 25 Apr 2015.
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
