

Effect of Tenapanor on Serum Phosphate in Patients Receiving Hemodialysis
- PMID: 28159782
- PMCID: PMC5461797
- DOI: 10.1681/ASN.2016080855
Effect of Tenapanor on Serum Phosphate in Patients Receiving Hemodialysis
Abstract
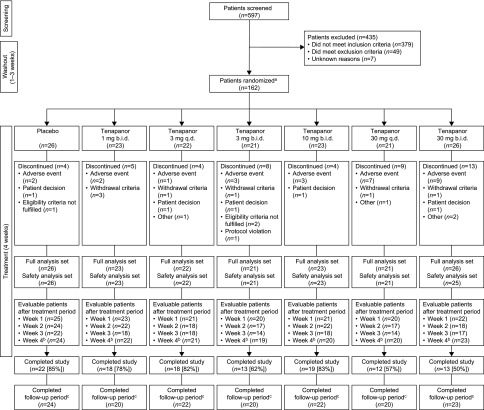
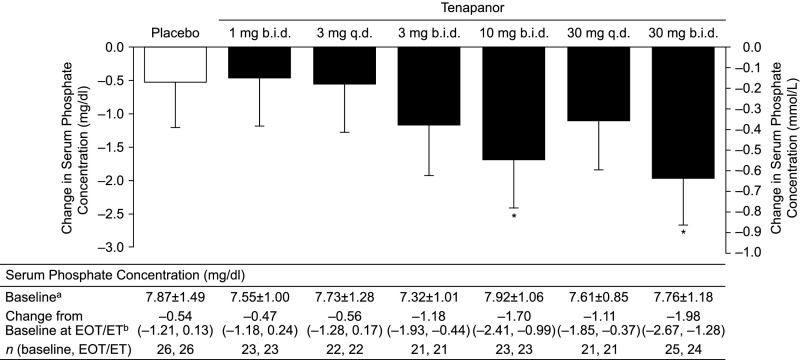
Hyperphosphatemia is common among patients with CKD stage 5D and is associated with morbidity and mortality. Current guidelines recommend lowering serum phosphate concentrations toward normal. Tenapanor is a minimally absorbed small molecule inhibitor of the sodium/hydrogen exchanger isoform 3 that functions in the gut to reduce sodium and phosphate absorption. This randomized, double-blind, placebo-controlled trial assessed the effects of tenapanor on serum phosphate concentration in patients with hyperphosphatemia receiving hemodialysis. After a 1- to 3-week washout of phosphate binders, we randomly assigned 162 eligible patients (serum phosphate =6.0 to <10.0 mg/dl and a 1.5-mg/dl increase from before washout) to one of six tenapanor regimens (3 or 30 mg once daily or 1, 3, 10, or 30 mg twice daily) or placebo for 4 weeks. The primary efficacy end point was change in serum phosphate concentration from baseline (randomization) to end of treatment. In total, 115 patients (71%) completed the study. Mean serum phosphate concentrations at baseline (after washout) were 7.32-7.92 mg/dl for tenapanor groups and 7.87 mg/dl for the placebo group. Tenapanor provided dose-dependent reductions in serum phosphate level from baseline (least squares mean change: tenapanor =0.47-1.98 mg/dl; placebo =0.54 mg/dl; P=0.01). Diarrhea was the most common adverse event (tenapanor =18%-68%; placebo =12%) and frequent at the highest tenapanor doses. In conclusion, tenapanor treatment resulted in statistically significant, dose-dependent reductions in serum phosphate concentrations in patients with hyperphosphatemia receiving hemodialysis. Additional studies are required to clarify the optimal dosing of tenapanor in patients with CKD-related hyperphosphatemia.
Keywords: NHE3; chronic kidney disease; hemodialysis; hyperphosphatemia; sodium–hydrogen exchanger 3; tenapanor.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Block GA, Hulbert-Shearon TE, Levin NW, Port FK: Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients: A national study. Am J Kidney Dis 31: 607–617, 1998 - PubMed
-
- Tonelli M, Pannu N, Manns B: Oral phosphate binders in patients with kidney failure. N Engl J Med 362: 1312–1324, 2010 - PubMed
-
- Tentori F, Blayney MJ, Albert JM, Gillespie BW, Kerr PG, Bommer J, Young EW, Akizawa T, Akiba T, Pisoni RL, Robinson BM, Port FK: Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 52: 519–530, 2008 - PubMed
-
- Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM: Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol 15: 2208–2218, 2004 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
