

Bevacizumab May Differentially Improve Ovarian Cancer Outcome in Patients with Proliferative and Mesenchymal Molecular Subtypes
- PMID: 28159814
- PMCID: PMC5661884
- DOI: 10.1158/1078-0432.CCR-16-2196
Bevacizumab May Differentially Improve Ovarian Cancer Outcome in Patients with Proliferative and Mesenchymal Molecular Subtypes
Abstract
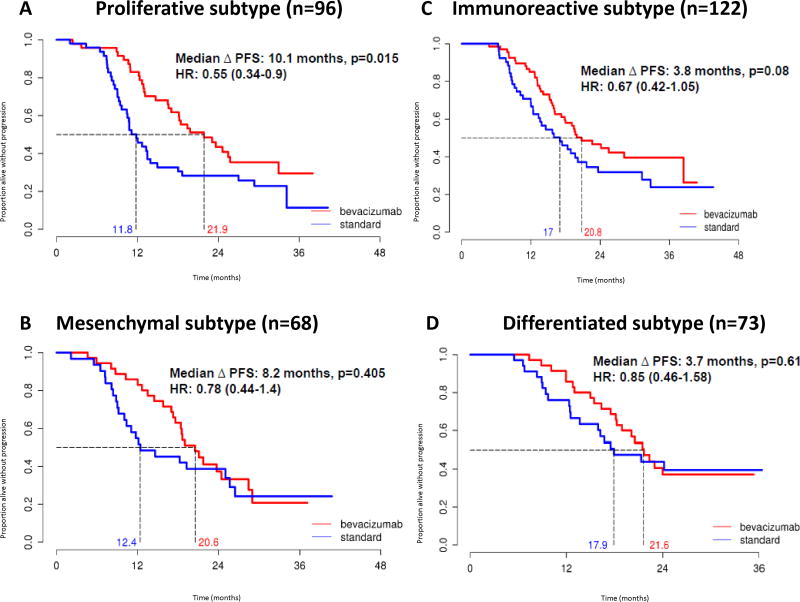
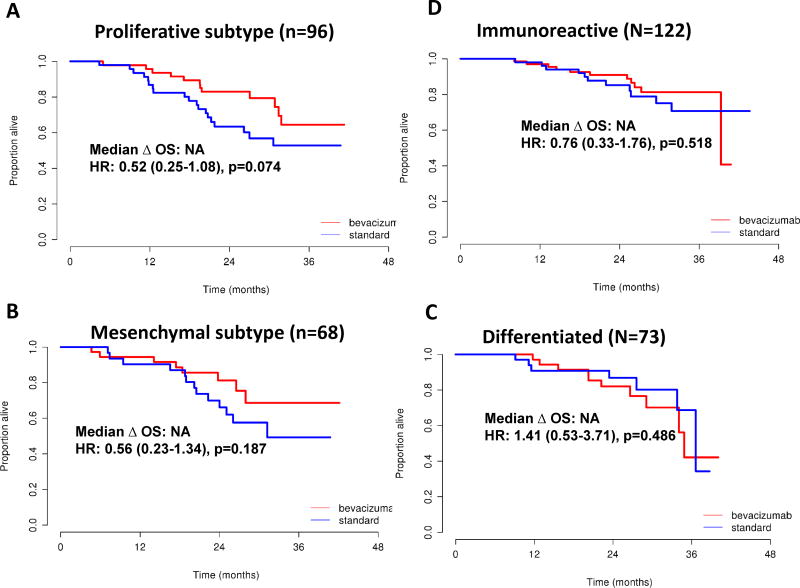
Purpose: Recent progress in understanding the molecular biology of epithelial ovarian cancer has not yet translated into individualized treatment for these women or improvements in their disease outcome. Gene expression has been utilized to identify distinct molecular subtypes, but there have been no reports investigating whether or not molecular subtyping is predictive of response to bevacizumab in ovarian cancer.Experimental Design: DASL gene expression arrays were performed on FFPE tissue from patients enrolled on the ICON7 trial. Patients were stratified into four TCGA molecular subtypes. Associations between molecular subtype and the efficacy of randomly assigned therapy with bevacizumab were assessed.Results: Molecular subtypes were assigned as follows: 122 immunoreactive (34%), 96 proliferative (27%), 73 differentiated (20%), and 68 mesenchymal (19%). In univariate analysis patients with tumors of proliferative subtype obtained the greatest benefit from bevacizumab with a median PFS improvement of 10.1 months [HR, 0.55 (95% CI, 0.34-0.90), P = 0.016]. For the mesenchymal subtype, bevacizumab conferred a nonsignificant improvement in PFS of 8.2 months [HR 0.78 (95% CI, 0.44-1.40), P = 0.41]. Bevacizumab conferred modest improvements in PFS for patients with immunoreactive subtype (3.8 months; P = 0.08) or differentiated subtype (3.7 months; P = 0.61). Multivariate analysis demonstrated significant PFS improvement in proliferative subtype patients only [HR, 0.45 (95% CI, 0.27-0.74), P = 0.0015].Conclusions: Ovarian carcinoma molecular subtypes with the poorest survival (proliferative and mesenchymal) derive a comparably greater benefit from treatment that includes bevacizumab. Validation of our findings in an independent cohort could enable the use of bevacizumab for those patients most likely to benefit, thereby reducing side effects and healthcare cost. Clin Cancer Res; 23(14); 3794-801. ©2017 AACR.
©2017 American Association for Cancer Research.
Conflict of interest statement
Stefan Kommoss (SK): Roche - consultancy, honoraria; AstraZeneca - honoraria.
Boris Winterhoff (BW): No conflicts of interest.
Ann L. Oberg (ALO): No conflicts of interest.
Gottfried E. Konecny (GEK): Genentech, Consulting; Amgen, Novartis, Research funding
Chen Wang (CW): No conflicts of interest.
Shaun M. Riska (SMR): No conflicts of interest.
Matthew J. Maurer (MJM): No conflicts of interest.
Jian-Bing Fan (JBF): No conflicts of interest.
Craig April (CA): I am an employee and shareholder of Illumina Inc.
Viji Shridhar (VS): No conflicts of interest.
Friedrich Kommoss (FK): No conflicts of interest.
Andreas du Bois (ADB): Personal fees from Roche, MSD, Astra Zeneca, Pharmamar and Amgen.
Felix Hilpert (FH): No conflicts of interest.
Sven Mahner (SM): Roche: Research support, Advisory Board, Honoraria, Travel Support; AstraZeneca: Research support, Advisory Board, Honoraria, Travel Support; Boehringer Ingelheim: Research support, Advisory Board, Travel Support; GlaxoSmithKline: Research support, Advisory Board, Honoraria, Travel Support
Klaus Baumann (KB): Tesaro – advisory board honoraria.
Willibald Schroeder (WS): No conflicts of interest.
Alexander Burges (AB): No conflicts of interest.
Ulrich Canzler (UC): Roche – honoraria.
Jeremy Chien (JC): No conflicts of interest.
Andrew C. Embleton (ACE): No conflicts of interest.
Mahesh Parmar (MP): No conflicts of interest.
Richard Kaplan (RK): No conflicts of interest.
Timothy Perren (TP): No conflicts of interest.
Lynn C. Hartmann (LCH): No conflicts of interest.
Ellen L. Goode (ELG): No conflicts of interest.
Sean C. Dowdy (SCD): No conflicts of interest.
Jacobus Pfisterer (JP): Speakers honoraria from Roche.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015 CA Cancer. J. Clin. 2015;65:5–29. - PubMed
-
- Tothill RW, Tinker AV, George J, Brown R, Fox SB, Lade S, et al. Novel molecular subtypes of serous and endometrioid ovarian cancer linked to clinical outcome. Clinical cancer research. 2008 Aug 15;14(16):5198–5208. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
