

Implications of Blood Pressure Measurement Technique for Implementation of Systolic Blood Pressure Intervention Trial (SPRINT)
- PMID: 28159816
- PMCID: PMC5523757
- DOI: 10.1161/JAHA.116.004536
Implications of Blood Pressure Measurement Technique for Implementation of Systolic Blood Pressure Intervention Trial (SPRINT)
Abstract
Background: Cardiovascular morbidity and mortality was reduced by 25% when blood pressure (BP) was targeted to 120 mm Hg systolic compared with 140 mm Hg systolic in Systolic Blood Pressure Intervention Trial (SPRINT); however, BP was measured using a research technique. SPRINT specified 5 minutes of seated rest in a quiet room followed by 3 oscillometric measurements without an observer in the room. The relationship of this research-grade methodology to routine BP measurements is not known.
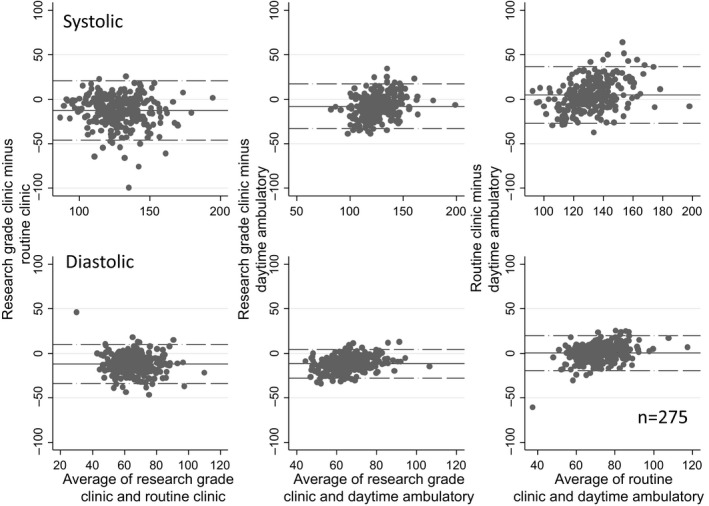
Methods and results: Among 275 people with chronic kidney disease who had BP <140/90 mm Hg when they came to the clinic, we measured BP as in SPRINT and recorded BP on the same day without specification of seated rest. Compared with routine measurement, the research-grade systolic BP was 12.7 mm Hg lower with wide limits of agreement (-46.1 to 20.7 mm Hg). Research grade systolic BP was 7.9 mm Hg lower than daytime ambulatory systolic BP and had wide agreement limits (-33.2 to 17.4 mm Hg). Whereas the routine, research-grade, and daytime ambulatory systolic BP were all related to echocardiographic left ventricular hypertrophy, the strength of the relationship between research-grade and daytime ambulatory systolic BP to left ventricular hypertrophy was similar and stronger than the strength of the relationship between routine systolic BP and left ventricular hypertrophy.
Conclusions: Taken together, these results suggest that translation of the SPRINT results will require measurement of BP as performed in that trial. Instead of an algebraic manipulation of routine clinic measurements, the SPRINT methodology of BP measurement would be needed at minimum if implementation of the SPRINT results were to be deployed in the population at large.
Keywords: agreement; ambulatory blood pressure monitoring; blood pressure measurement; chronic kidney disease; left ventricular hypertrophy.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures

References
-
- James PA, Oparil S, Carter BL, Cushman WC, Dennison‐Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 evidence‐based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–520. - PubMed
-
- Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, Reboussin DM, Rahman M, Oparil S, Lewis CE, Kimmel PL, Johnson KC, Goff DC Jr, Fine LJ, Cutler JA, Cushman WC, Cheung AK, Ambrosius WT. A randomized trial of intensive versus standard blood‐pressure control. N Engl J Med. 2015;373:2103–2116. - PMC - PubMed
-
- Williamson JD, Supiano MA, Applegate WB, Berlowitz DR, Campbell RC, Chertow GM, Fine LJ, Haley WE, Hawfield AT, Ix JH, Kitzman DW, Kostis JB, Krousel‐Wood MA, Launer LJ, Oparil S, Rodriguez CJ, Roumie CL, Shorr RI, Sink KM, Wadley VG, Whelton PK, Whittle J, Woolard NF, Wright JT Jr, Pajewski NM. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged >/=75 years: a randomized clinical trial. JAMA. 2016;315:2673–2682. - PMC - PubMed
-
- El Assaad MA, Topouchian JA, Darne BM, Asmar RG. Validation of the Omron HEM‐907 device for blood pressure measurement. Blood Press Monit. 2002;7:237–241. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
