

IgA Nephropathy
- PMID: 28159829
- PMCID: PMC5383386
- DOI: 10.2215/CJN.07420716
IgA Nephropathy
Abstract
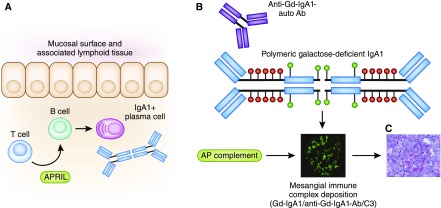
IgA nephropathy (IgAN) is a leading cause of CKD and renal failure. Recent international collaborative efforts have led to important discoveries that have improved our understanding of some of the key steps involved in the immunopathogenesis of IgAN. Furthermore, establishment of multicenter networks has contributed to rigorous design and execution of clinical trials that have provided important insights regarding immunotherapy in IgAN. In this article, we review emerging developments in clinical and translational IgAN research and describe how these novel findings will influence future strategies to improve the outcome of patients with IgAN.
Keywords: IGA; IgA nephropathy; chronic; corticosteroids; crescents; glomerulonephritis; humans; immunosuppression; immunotherapy; kidney; pathology; renal insufficiency; review; translational medical research.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- McGrogan A, Franssen CF, de Vries CS: The incidence of primary glomerulonephritis worldwide: A systematic review of the literature. Nephrol Dial Transplant 26: 414–430, 2011 - PubMed
-
- Sehic AM, Gaber LW, Roy S 3rd, Miller PM, Kritchevsky SB, Wyatt RJ: Increased recognition of IgA nephropathy in African-American children. Pediatr Nephrol 11: 435–437, 1997 - PubMed
-
- Utsunomiya Y, Koda T, Kado T, Okada S, Hayashi A, Kanzaki S, Kasagi T, Hayashibara H, Okasora T: Incidence of pediatric IgA nephropathy. Pediatr Nephrol 18: 511–515, 2003 - PubMed
-
- Suzuki K, Honda K, Tanabe K, Toma H, Nihei H, Yamaguchi Y: Incidence of latent mesangial IgA deposition in renal allograft donors in Japan. Kidney Int 63: 2286–2294, 2003 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
