

Optimizing Outpatient Pain Management After Thyroid and Parathyroid Surgery: A Two-Institution Experience
- PMID: 28160140
- PMCID: PMC5451307
- DOI: 10.1245/s10434-017-5781-y
Optimizing Outpatient Pain Management After Thyroid and Parathyroid Surgery: A Two-Institution Experience
Abstract
Background: Thyroidectomy and parathyroidectomy are the most commonly performed endocrine operations, and are increasingly being completed on a same-day basis; however, few data exist regarding the outpatient postoperative pain requirement of these patients. We aimed to describe the outpatient narcotic medication needs for patients undergoing thyroid and parathyroid surgery, and to identify predictors of higher requirement.
Method: We examined patients undergoing thyroid and parathyroid surgery at two large academic institutions from 1 January-30 May 2014. Prospective data were collected on pain scores and the oral morphine equivalents (OMEQs) taken by these patients by their postoperative visit.
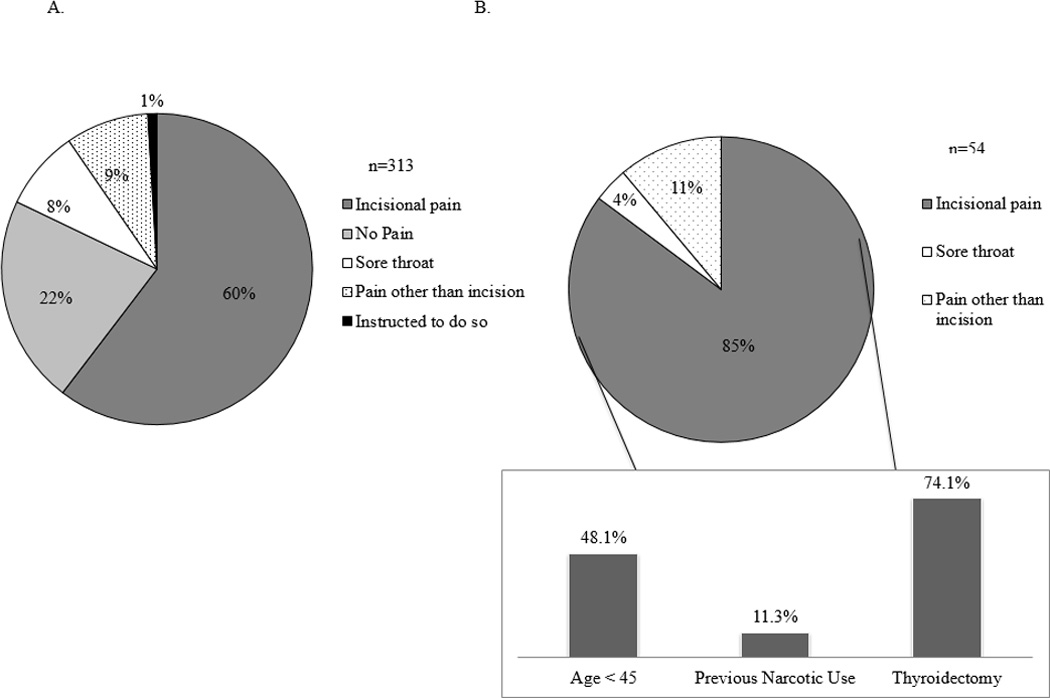
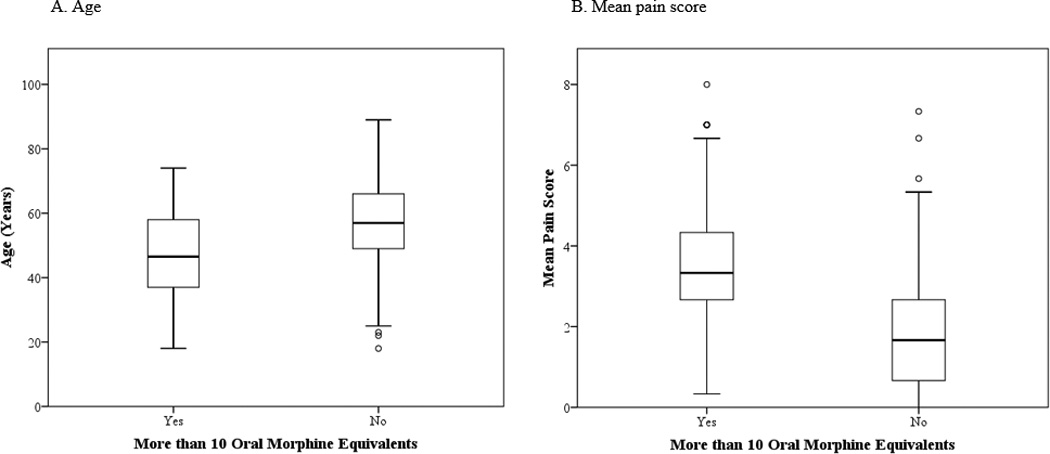
Results: Overall, 313 adult patients underwent thyroidectomy or parathyroidectomy during the study period; 83% of patients took ten or fewer OMEQs, and 93% took 20 or fewer OMEQs. Patients who took more than ten OMEQs were younger (p < 0.001) and reported significantly higher overall mean pain scores at their postoperative visit (p < 0.001) than patients who took fewer than ten OMEQs. A multivariate model was constructed on pre- and intraoperative factors that may predict use of more than ten OMEQs postoperatively. Age <45 years (p = 0.002), previous narcotic use (p = 0.037), and whether parathyroid or thyroid surgery was performed (p = 0.003) independently predicted the use of more than ten OMEQs after surgery. A subgroup analysis was then performed on thyroidectomy-only patients.
Conclusion: Overall, 93% of patients undergoing thyroidectomy and parathyroidectomy require 20 or fewer OMEQs by their postoperative visit. We therefore recommend these patients be discharged with 20 OMEQs, both to minimize waste and increase patient safety.
Conflict of interest statement
For the remaining authors, none are declared.
Figures

References
-
- Mowschenson PM, Hodin RA. Outpatient thyroid and parathyroid surgery: a prospective study of feasibility, safety, and costs. Surgery. 1995;118(6):1051–1053. discussion 1053-4. - PubMed
-
- Terris DJ, Snyder S, Carneiro-Pla D, et al. American Thyroid Association statement on outpatient thyroidectomy. Thyroid. 2013;23(10):1193–1202. - PubMed
-
- Irvin GL, Sfakianakis G, Yeung L, et al. Ambulatory parathyroidectomy for primary hyperparathyroidism. Arch Surg. 1996;131(10):1074–1078. - PubMed
-
- Flynn MB, Quayyum M, Goldstein RE, et al. Outpatient parathyroid surgery: ten-year experience: is it safe? Am Surg. 2015;81(5):472–477. - PubMed
-
- Egan RJ, Hopkins JC, Beamish AJ, et al. Randomized clinical trial of intraoperative superficial cervical plexus block versus incisional local anaesthesia in thyroid and parathyroid surgery. Br J Surg. 2013;100(13):1732–1738. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
