

Meta-analysis of individual-patient data from EVAR-1, DREAM, OVER and ACE trials comparing outcomes of endovascular or open repair for abdominal aortic aneurysm over 5 years
- PMID: 28160528
- PMCID: PMC5299468
- DOI: 10.1002/bjs.10430
Meta-analysis of individual-patient data from EVAR-1, DREAM, OVER and ACE trials comparing outcomes of endovascular or open repair for abdominal aortic aneurysm over 5 years
Erratum in
-
Corrigenda.Br J Surg. 2018 Aug;105(9):1222. doi: 10.1002/bjs.10928. Br J Surg. 2018. PMID: 30461004 Free PMC article. No abstract available.
Abstract
Background: The erosion of the early mortality advantage of elective endovascular aneurysm repair (EVAR) compared with open repair of abdominal aortic aneurysm remains without a satisfactory explanation.
Methods: An individual-patient data meta-analysis of four multicentre randomized trials of EVAR versus open repair was conducted to a prespecified analysis plan, reporting on mortality, aneurysm-related mortality and reintervention.
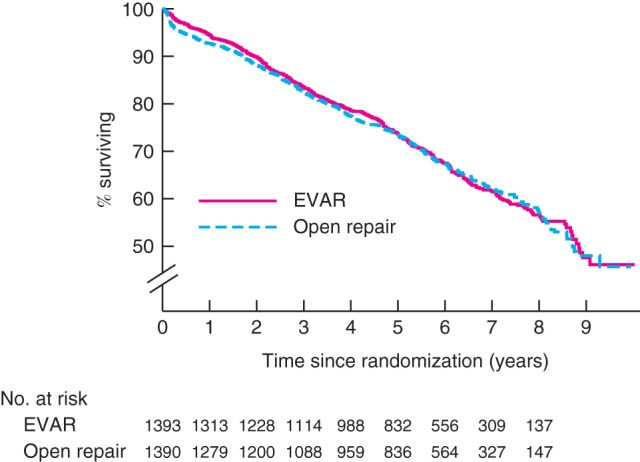
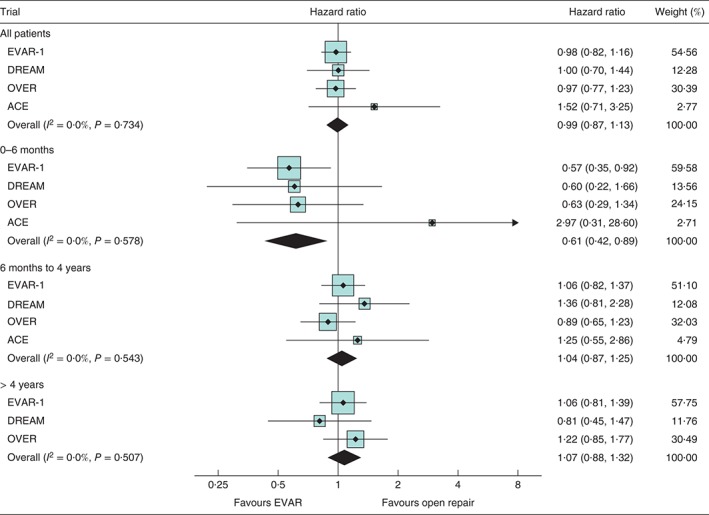
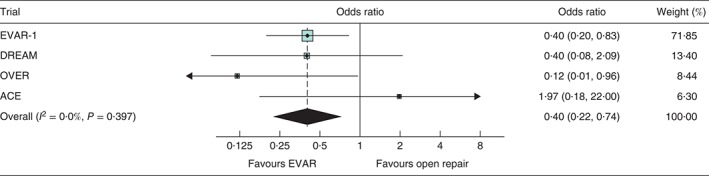
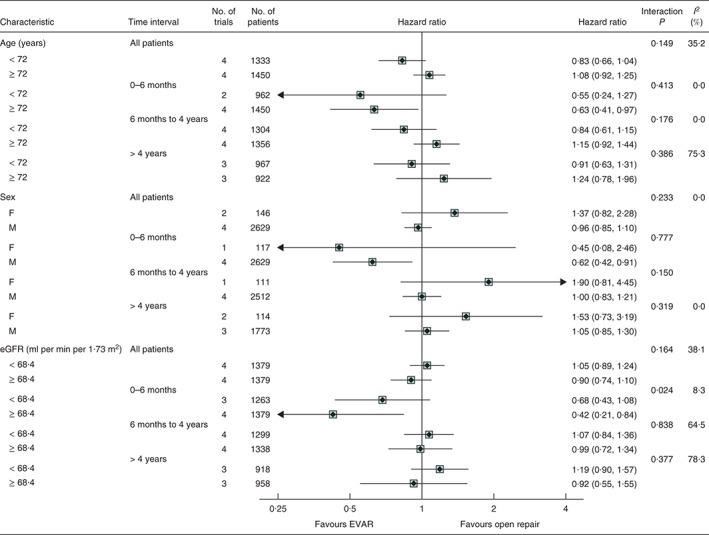
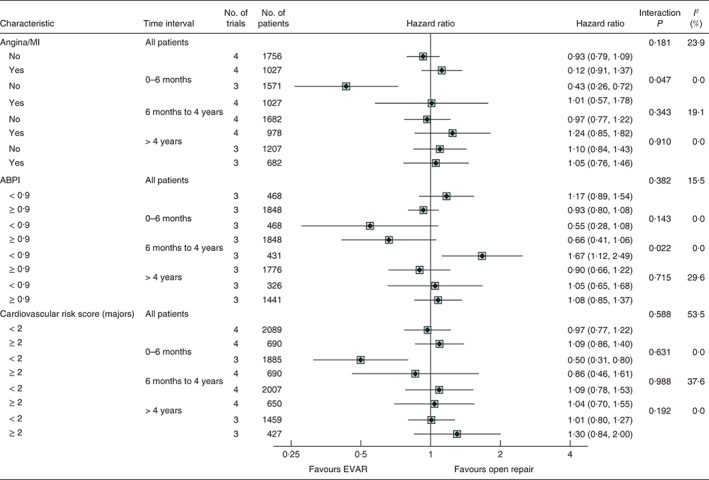
Results: The analysis included 2783 patients, with 14 245 person-years of follow-up (median 5·5 years). Early (0-6 months after randomization) mortality was lower in the EVAR groups (46 of 1393 versus 73 of 1390 deaths; pooled hazard ratio 0·61, 95 per cent c.i. 0·42 to 0·89; P = 0·010), primarily because 30-day operative mortality was lower in the EVAR groups (16 deaths versus 40 for open repair; pooled odds ratio 0·40, 95 per cent c.i. 0·22 to 0·74). Later (within 3 years) the survival curves converged, remaining converged to 8 years. Beyond 3 years, aneurysm-related mortality was significantly higher in the EVAR groups (19 deaths versus 3 for open repair; pooled hazard ratio 5·16, 1·49 to 17·89; P = 0·010). Patients with moderate renal dysfunction or previous coronary artery disease had no early survival advantage under EVAR. Those with peripheral artery disease had lower mortality under open repair (39 deaths versus 62 for EVAR; P = 0·022) in the period from 6 months to 4 years after randomization.
Conclusion: The early survival advantage in the EVAR group, and its subsequent erosion, were confirmed. Over 5 years, patients of marginal fitness had no early survival advantage from EVAR compared with open repair. Aneurysm-related mortality and patients with low ankle : brachial pressure index contributed to the erosion of the early survival advantage for the EVAR group. Trial registration numbers: EVAR-1, ISRCTN55703451; DREAM (Dutch Randomized Endovascular Aneurysm Management), NCT00421330; ACE (Anévrysme de l'aorte abdominale, Chirurgie versus Endoprothèse), NCT00224718; OVER (Open Versus Endovascular Repair Trial for Abdominal Aortic Aneurysms), NCT00094575.
© 2017 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Dubost C, Allary M, Oeconomos N. [Treatment of aortic aneurysms; removal of the aneurysm; re‐establishment of continuity by grafts of preserved human aorta.] Mem Acad Chir (Paris) 1951; 77: 381–383. - PubMed
-
- Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG; EVAR trial participants. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30‐day operative mortality results: randomised controlled trial. Lancet 2004; 364: 843–848. - PubMed
-
- Blankensteijn JD, de Jong SE, Prinssen M, van der Ham AC, Buth J, van Sterkenburg SM et al; Dutch Randomized Endovascular Aneurysm Management (DREAM) Trial Group. Two‐year outcomes after conventional or endovascular repair of abdominal aortic aneurysms. N Engl J Med 2005; 352: 2398–2405. - PubMed
-
- Becquemin JP, Pillet JC, Lescalie F, Sapoval M, Goueffic Y, Lermusiaux P et al; ACE trialists. A randomized controlled trial of endovascular aneurysm repair versus open surgery for abdominal aortic aneurysms in low‐to‐moderate‐risk patients. J Vasc Surg 2011; 53: 1167–1173. - PubMed
-
- Lederle FA, Freischlag JA, Kyriakides TC, Matsumura JS, Padberg FT Jr, Kohler TR et al; OVER Veterans Affairs Cooperative Study Group. Long‐term comparison of endovascular and open repair of abdominal aortic aneurysm. N Engl J Med 2012; 367: 1988–1997. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
