

Elbow Instability: Anatomy, Biomechanics, Diagnostic Maneuvers, and Testing
- PMID: 28160902
- PMCID: PMC5821063
- DOI: 10.1016/j.jhsa.2016.11.025
Elbow Instability: Anatomy, Biomechanics, Diagnostic Maneuvers, and Testing
Abstract
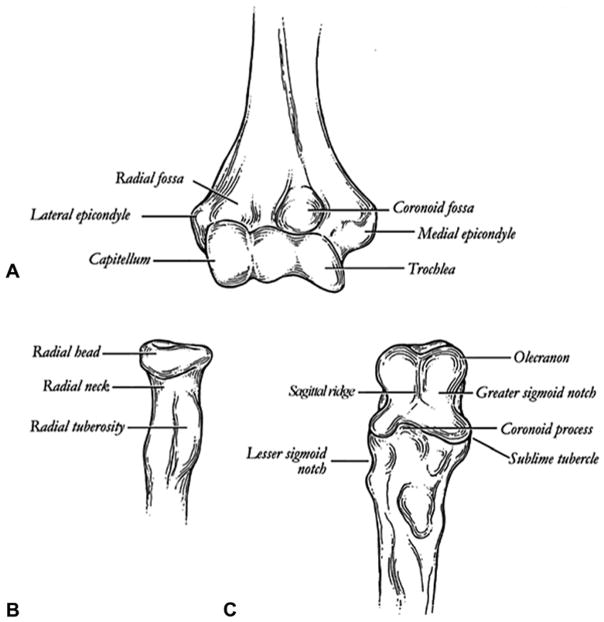
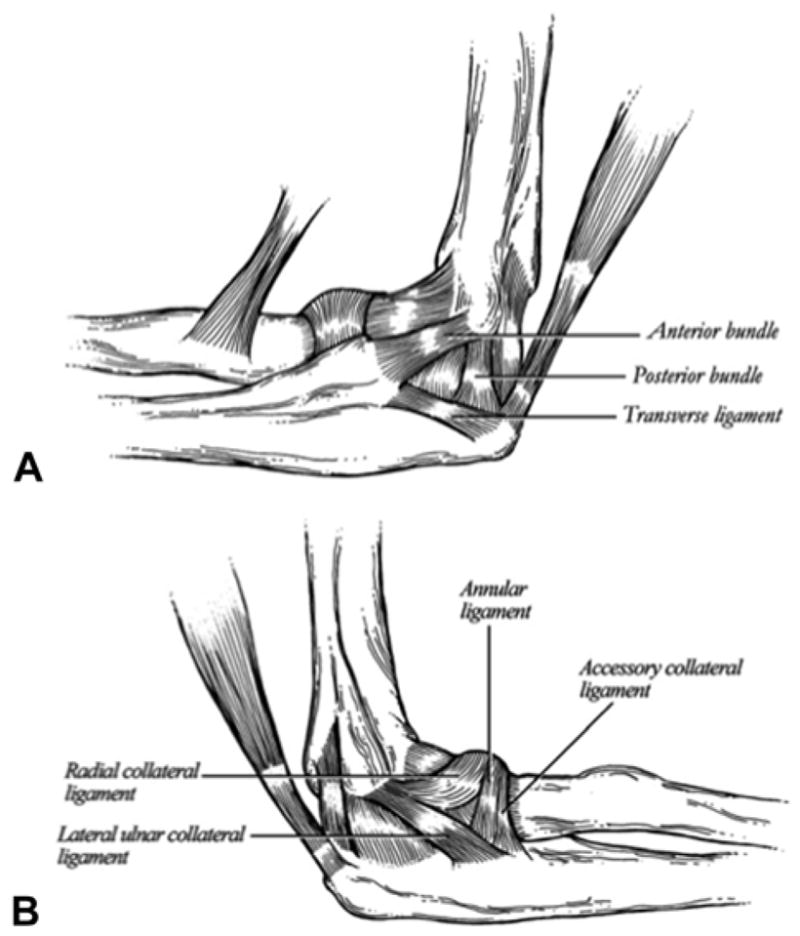
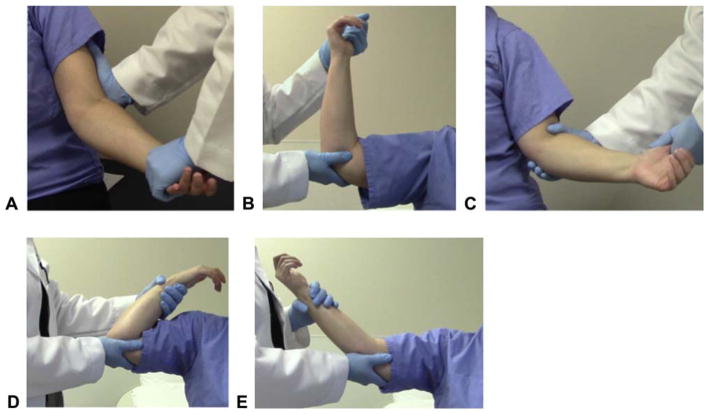
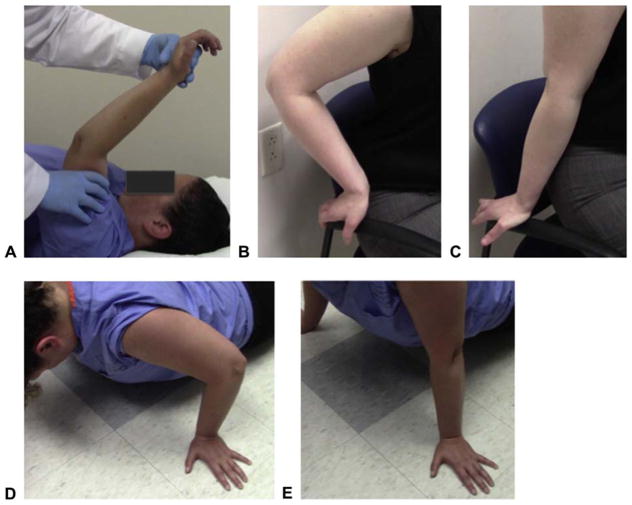
The elbow comprises a complex of bony and ligamentous stabilizers that provide both primary and secondary constraints to elbow instability. Through trauma and overuse, classic instability patterns arise by loss of these important stabilizers. The diagnosis of elbow instability can made using specific examination maneuvers and testing to diagnose the clinical pattern. This article reviews the elbow's unique anatomy and biomechanical characteristics and these are applied when reviewing the maneuvers and testing used to diagnose elbow instability.
Keywords: Valgus instability; elbow biomechanics; posterolateral rotatory instability; varus posteromedial rotatory instability.
Copyright © 2017 American Society for Surgery of the Hand. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Hausman MR, Lang P. Examination of the elbow: current concepts. J Hand Surg Am. 2014;39(12):2534–2541. - PubMed
-
- Bryce CD, Armstrong AD. Anatomy and biomechanics of the elbow. Orthop Clin North Am. 2008;39(2):141–154. v. - PubMed
-
- Morrey BF, An KN. Stability of the elbow: osseous constraints. J Shoulder Elbow Surg. 2005;14(1 Suppl S):174S–178S. - PubMed
-
- Ahmed I, Mistry J. The management of acute and chronic elbow instability. Orthop Clin North Am. 2015;46(2):271–280. - PubMed
-
- Safran MR, Baillargeon D. Soft-tissue stabilizers of the elbow. J Shoulder Elbow Surg. 2005;14(1 Suppl S):179S–185S. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
