

Single-Center Experience with a Targeted Next Generation Sequencing Assay for Assessment of Relevant Somatic Alterations in Solid Tumors
- PMID: 28161563
- PMCID: PMC5293722
- DOI: 10.1016/j.neo.2017.01.003
Single-Center Experience with a Targeted Next Generation Sequencing Assay for Assessment of Relevant Somatic Alterations in Solid Tumors
Abstract
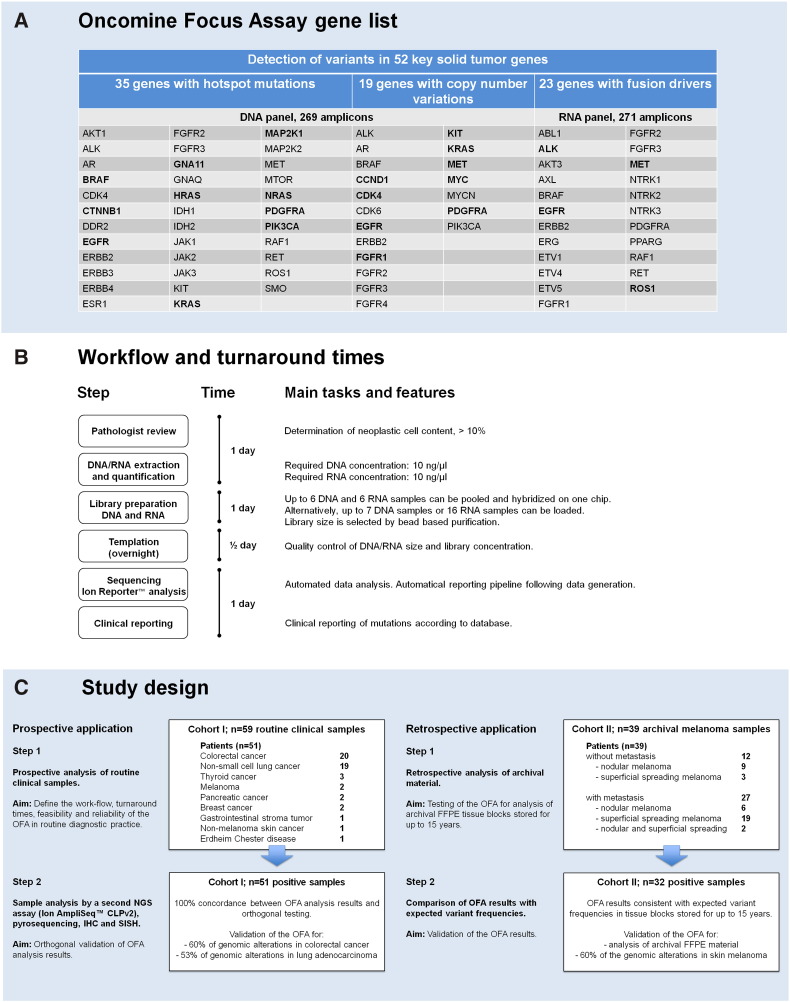
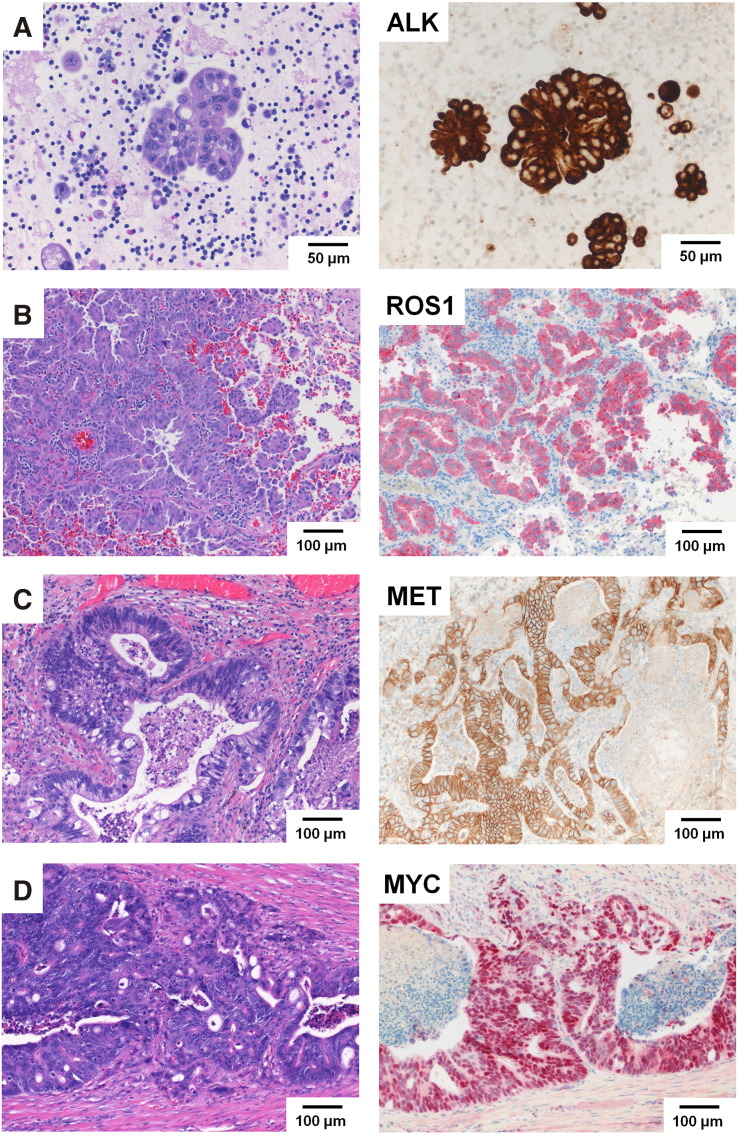
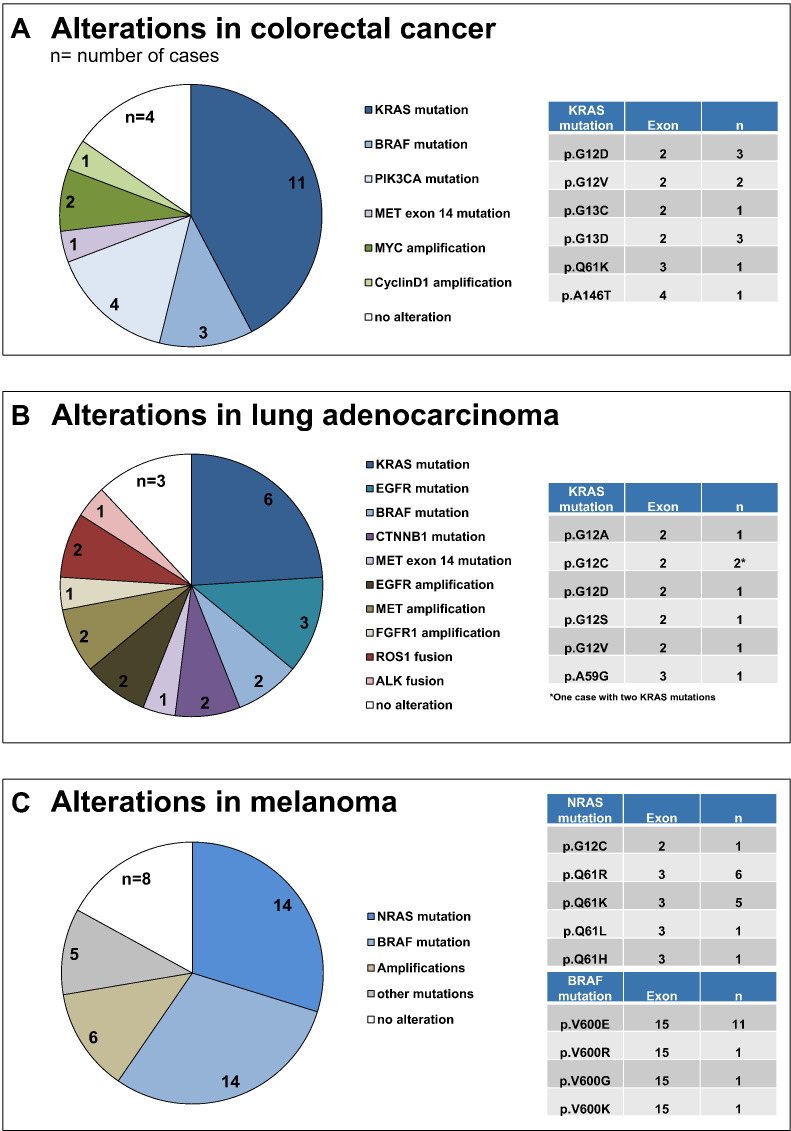
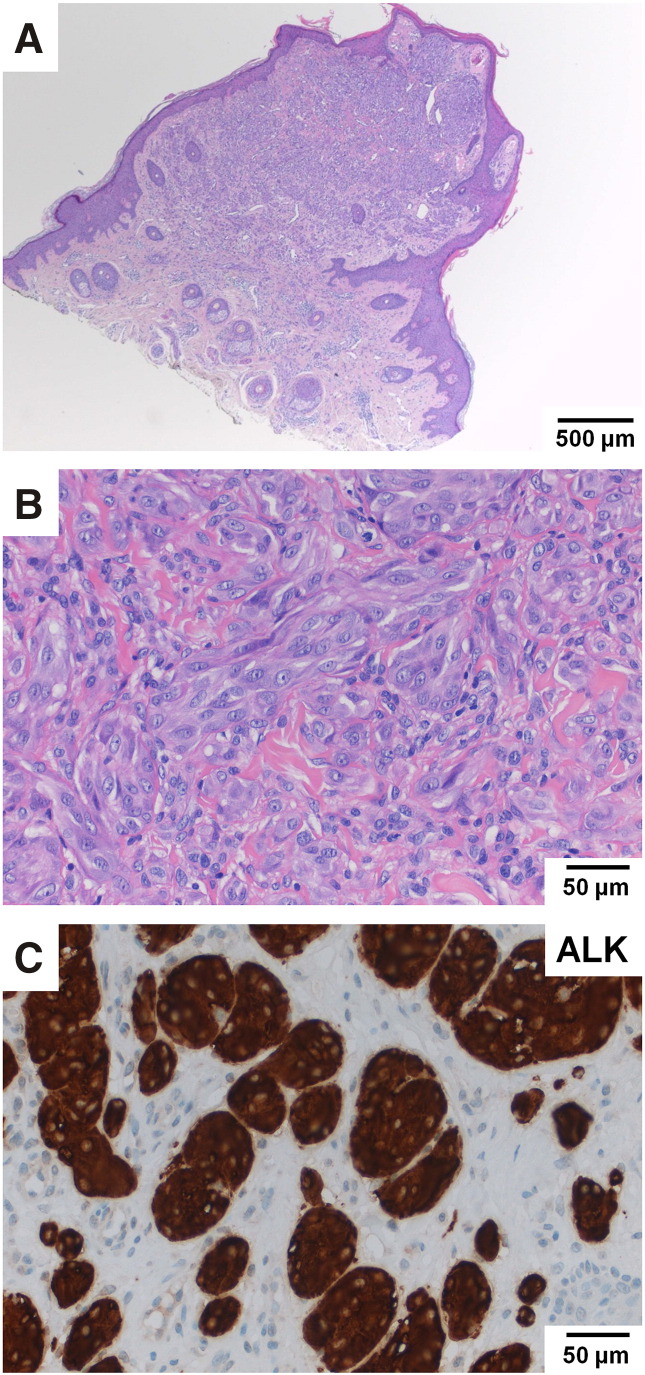
Companion diagnostics rely on genomic testing of molecular alterations to enable effective cancer treatment. Here we report the clinical application and validation of the Oncomine Focus Assay (OFA), an integrated, commercially available next-generation sequencing (NGS) assay for the rapid and simultaneous detection of single nucleotide variants, short insertions and deletions, copy number variations, and gene rearrangements in 52 cancer genes with therapeutic relevance. Two independent patient cohorts were investigated to define the workflow, turnaround times, feasibility, and reliability of OFA targeted sequencing in clinical application and using archival material. Cohort I consisted of 59 diagnostic clinical samples from the daily routine submitted for molecular testing over a 4-month time period. Cohort II consisted of 39 archival melanoma samples that were up to 15years old. Libraries were prepared from isolated nucleic acids and sequenced on the Ion Torrent PGM sequencer. Sequencing datasets were analyzed using the Ion Reporter software. Genomic alterations were identified and validated by orthogonal conventional assays including pyrosequencing and immunohistochemistry. Sequencing results of both cohorts, including archival formalin-fixed, paraffin-embedded material stored up to 15years, were consistent with published variant frequencies. A concordance of 100% between established assays and OFA targeted NGS was observed. The OFA workflow enabled a turnaround of 3½ days. Taken together, OFA was found to be a convenient tool for fast, reliable, broadly applicable and cost-effective targeted NGS of tumor samples in routine diagnostics. Thus, OFA has strong potential to become an important asset for precision oncology.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
