

Mindfulness and pharmacological prophylaxis after withdrawal from medication overuse in patients with Chronic Migraine: an effectiveness trial with a one-year follow-up
- PMID: 28161874
- PMCID: PMC5292107
- DOI: 10.1186/s10194-017-0728-z
Mindfulness and pharmacological prophylaxis after withdrawal from medication overuse in patients with Chronic Migraine: an effectiveness trial with a one-year follow-up
Abstract
Background: Chronic Migraine (CM) is a disabling condition, worsened when associated with Medication Overuse (MO). Mindfulness is an emerging technique, effective in different pain conditions, but it has yet to be explored for CM-MO. We report the results of a study assessing a one-year course of patients' status, with the hypothesis that the effectiveness of a mindfulness-based approach would be similar to that of conventional prophylactic treatments.
Methods: Patients with CM-MO (code 1.3 and 8.2 of the International Classification of Headache Disorders-3Beta) completed a withdrawal program in a day hospital setting. After withdrawal, patients were either treated with Prophylactic Medications (Med-Group), or participated in a Mindfulness-based Training (MT-Group). MT consisted of 6 weekly sessions of guided mindfulness, with patients invited to practice 7-10 min per day. Headache diaries, the headache impact test (HIT-6), the migraine disability assessment (MIDAS), state and trait anxiety (STAI Y1-Y2), and the Beck Depression Inventory (BDI) were administered before withdrawal and at each follow-up (3, 6, 12 after withdrawal) to patients from both groups. Outcome variables were analyzed in separate two-way mixed ANOVAs (Group: Mindfulness vs. Pharmacology x Time: Baseline, 3-, 6-, vs. 12-month follow-up).
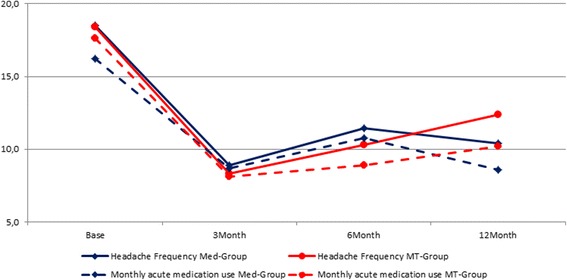
Results: A total of 44 patients participated in the study, with the average age being 44.5, average headache frequency/month was 20.5, and average monthly medication intake was 18.4 pills. Data revealed a similar improvement over time in both groups for Headache Frequency (approximately 6-8 days reduction), use of Medication (approximately 7 intakes reduction), MIDAS, HIT-6 (but only for the MED-Group), and BDI; no changes on state and trait anxiety were found. Both groups revealed significant and equivalent improvement with respect to what has become a classical endpoint in this area of research, i.e. 50% or more reduction of headaches compared to baseline, and the majority of patients in each condition no longer satisfied current criteria for CM.
Conclusions: Taken as a whole, our results suggest that the longitudinal course of patients in the MT-Group, that were not prescribed medical prophylaxis, was substantially similar to that of patients who were administered medical prophylaxis.
Keywords: Chronic migraine; Medication overuse; Mindfulness; Pharmacological prophylaxis.
Figures


Similar articles
-
A prospective pilot study of the effect on catecholamines of mindfulness training vs pharmacological prophylaxis in patients with chronic migraine and medication overuse headache.Cephalalgia. 2019 Apr;39(5):655-664. doi: 10.1177/0333102418801584. Epub 2018 Sep 13. Cephalalgia. 2019. PMID: 30213202 Clinical Trial.
-
Mindfulness and pharmacological prophylaxis have comparable effect on biomarkers of inflammation and clinical indexes in chronic migraine with medication overuse: results at 12 months after withdrawal.Neurol Sci. 2017 May;38(Suppl 1):173-175. doi: 10.1007/s10072-017-2874-0. Neurol Sci. 2017. PMID: 28527073
-
Efficacy of mindfulness added to treatment as usual in patients with chronic migraine and medication overuse headache: a phase-III single-blind randomized-controlled trial (the MIND-CM study).J Headache Pain. 2023 Jul 14;24(1):86. doi: 10.1186/s10194-023-01630-0. J Headache Pain. 2023. PMID: 37452281 Free PMC article. Clinical Trial.
-
Chronic migraine: current concepts and ongoing treatments.Eur Rev Med Pharmacol Sci. 2011 Dec;15(12):1401-20. Eur Rev Med Pharmacol Sci. 2011. PMID: 22288302 Review.
-
Medication overuse and chronic migraine: a critical review according to clinical pharmacology.Expert Opin Drug Metab Toxicol. 2015 Jul;11(7):1127-44. doi: 10.1517/17425255.2015.1043265. Epub 2015 May 31. Expert Opin Drug Metab Toxicol. 2015. PMID: 26027878 Review.
Cited by
-
A Preliminary Analysis on the Feasibility and Short-Term Efficacy of a Phase-III RCT on Mindfulness Added to Treatment as Usual for Patients with Chronic Migraine and Medication Overuse Headache.Int J Environ Res Public Health. 2022 Oct 29;19(21):14116. doi: 10.3390/ijerph192114116. Int J Environ Res Public Health. 2022. PMID: 36360996 Free PMC article. Clinical Trial.
-
Exploring Emotional Distress, Psychological Traits and Attitudes in Patients with Chronic Migraine Undergoing OnabotulinumtoxinA Prophylaxis versus Withdrawal Treatment.Toxins (Basel). 2020 Sep 8;12(9):577. doi: 10.3390/toxins12090577. Toxins (Basel). 2020. PMID: 32911799 Free PMC article.
-
The Role of the Person Focused IARA Model in Reducing Anxiety and Improving Body Awareness and Illness Management in Diabetics with Acquired Lipodystrophy: A Mixed-Method Study.J Pers Med. 2022 Nov 8;12(11):1865. doi: 10.3390/jpm12111865. J Pers Med. 2022. PMID: 36579585 Free PMC article.
-
Medication-overuse headache-a review of different treatment strategies.Front Pain Res (Lausanne). 2023 Oct 10;4:1103497. doi: 10.3389/fpain.2023.1103497. eCollection 2023. Front Pain Res (Lausanne). 2023. PMID: 37881687 Free PMC article. Review.
-
Meditative and Mindfulness-Focused Interventions in Neurology: Principles, Science, and Patient Selection.Semin Neurol. 2022 Apr;42(2):123-135. doi: 10.1055/s-0042-1742287. Epub 2022 Feb 9. Semin Neurol. 2022. PMID: 35139550 Free PMC article.
References
-
- Global Burden of Disease Study 2013 Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. doi: 10.1016/S0140-6736(15)60692-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
