

The influence of innate and adaptative immune responses on the differential clinical outcomes of leprosy
- PMID: 28162092
- PMCID: PMC5292790
- DOI: 10.1186/s40249-016-0229-3
The influence of innate and adaptative immune responses on the differential clinical outcomes of leprosy
Abstract
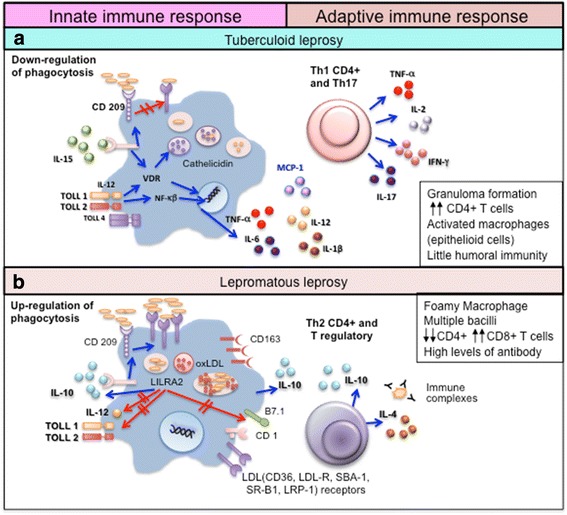
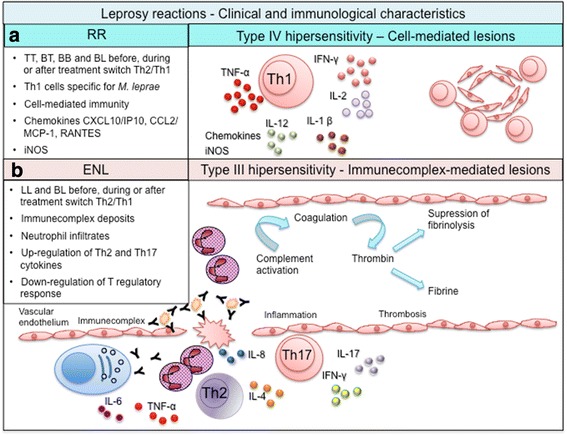
Leprosy is a chronic infectious disease caused by Mycobacterium leprae. According to official reports from 121 countries across five WHO regions, there were 213 899 newly diagnosed cases in 2014. Although leprosy affects the skin and peripheral nerves, it can present across a spectrum of clinical and histopathological forms that are strongly influenced by the immune response of the infected individuals. These forms comprise the extremes of tuberculoid leprosy (TT), with a M. leprae-specific Th1, but also a Th17, response that limits M. leprae multiplication, through to lepromatous leprosy (LL), with M. leprae-specific Th2 and T regulatory responses that do not control M. leprae replication but rather allow bacterial dissemination. The interpolar borderline clinical forms present with similar, but less extreme, immune biases. Acute inflammatory episodes, known as leprosy reactions, are complications that may occur before, during or after treatment, and cause further neurological damages that can cause irreversible chronic disabilities. This review discusses the innate and adaptive immune responses, and their interactions, that are known to affect pathogenesis and influence the clinical outcome of leprosy.
Keywords: Clinical presentation; Immune pathogenesis; Immunology; Innate immunity; Leprosy.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
