

Airway and serum biochemical correlates of refractory neutrophilic asthma
- PMID: 28163052
- PMCID: PMC5540819
- DOI: 10.1016/j.jaci.2016.12.963
Airway and serum biochemical correlates of refractory neutrophilic asthma
Abstract
Background: Despite progress in the diagnosis and management of asthma, many patients have poorly controlled or refractory asthma (RA). The mechanism of this RA is not well understood.
Objective: We sought to explore the relationship between neutrophils and other biomarkers of RA.
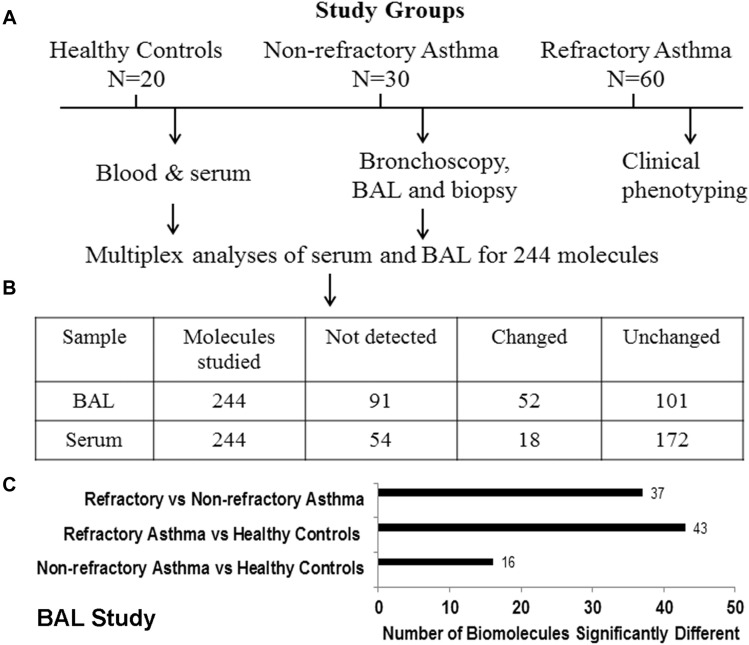
Method: Sixty patients with RA, 30 patients with nonrefractory asthma (NRA), and 20 healthy subjects were enrolled. We performed a comprehensive characterization of these study subjects, which included laboratory and pulmonary function studies, chest computed tomography, and bronchoscopy with bronchoalveolar lavage (BAL). We analyzed BAL fluid and serum for a total of 244 biomolecules using a multiplex assay and correlated them with clinical and other laboratory parameters.
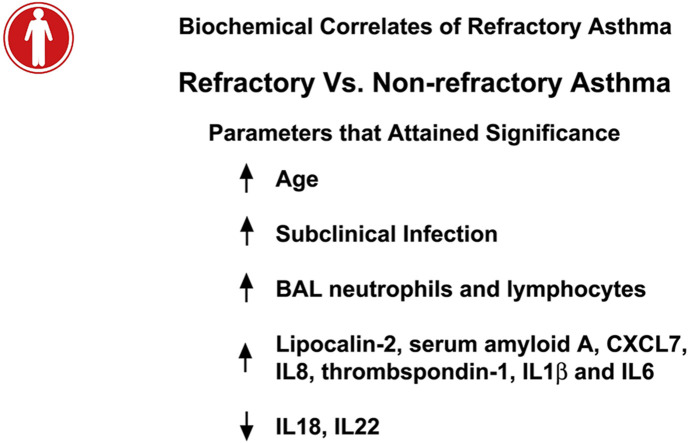
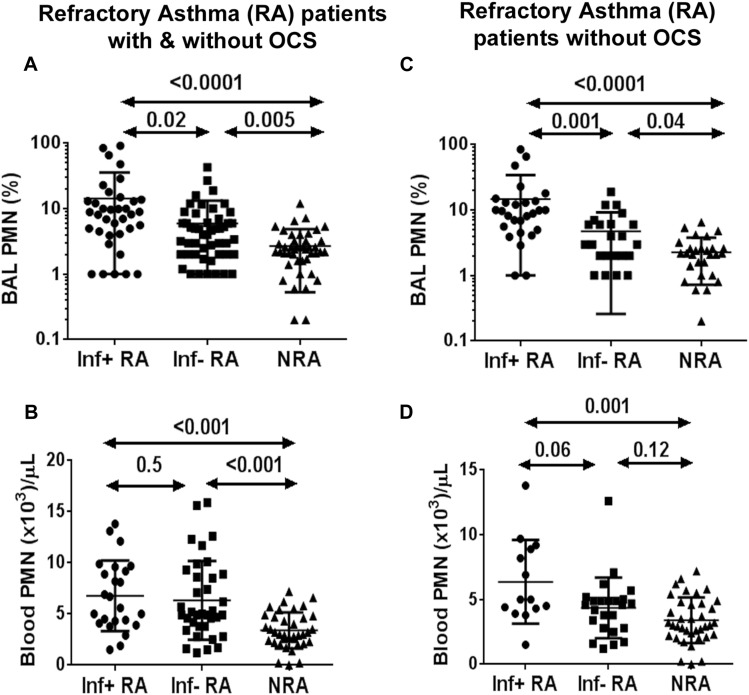
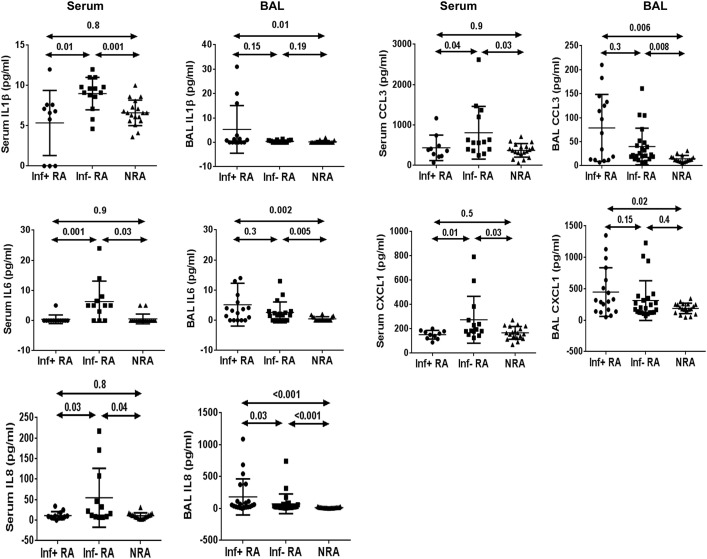
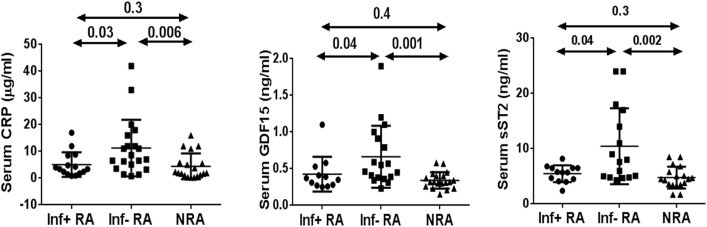
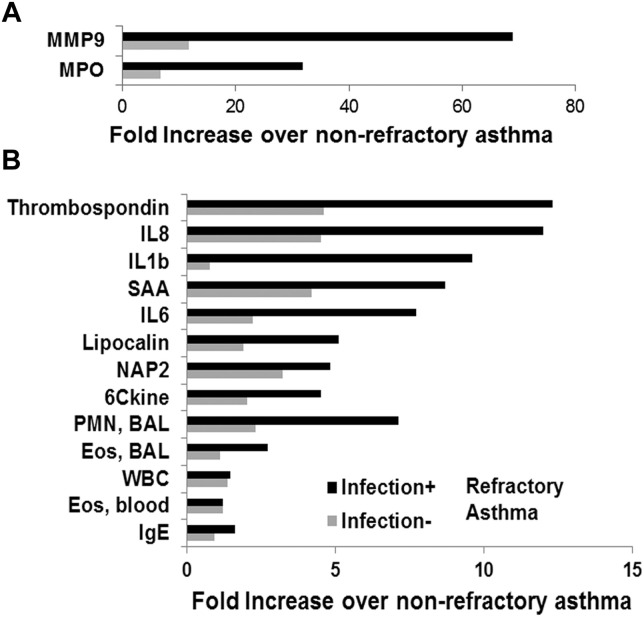
Results: RA was significantly different from NRA with regard to pulmonary function indices, bronchial basement membrane thickness, and BAL fluid neutrophil and lymphocyte counts but not eosinophil counts. BAL fluid neutrophil counts negatively and positively correlated with forced vital capacity and age, respectively. Of the 244 biomolecules studied, 52 and 14 biomolecules from BAL fluid and serum, respectively, were significantly different among the study groups. Thirteen of these 52 molecules correlated with BAL fluid neutrophil counts. BAL fluid from 40% of patients with RA was positive for a pathogenic microbe. Infection-negative neutrophilic RA was associated with an increase in levels of select biomarkers of inflammation in the serum, suggesting the presence of systemic inflammation.
Conclusions: RA was associated with increased numbers of neutrophils and proneutrophilic biomolecules in the airways. Subclinical infection was present in 40% of patients with RA, which likely contributed to neutrophilic inflammation. A subgroup of patients with noninfected neutrophilic RA was associated with systemic inflammation.
Keywords: Refractory asthma; bronchoalveolar lavage; cytokines; infection; neutrophilic asthma.
Copyright © 2017 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Chung K.F., Wenzel S.E., Brozek J.L., Bush A., Castro M., Sterk P.J. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43:343–373. - PubMed
-
- Wenzel S.E. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med. 2012;18:716–725. - PubMed
-
- Hekking P.P., Wener R.R., Amelink M., Zwinderman A.H., Bouvy M.L., Bel E.H. The prevalence of severe refractory asthma. J Allergy Clin Immunol. 2015;135:896–902. - PubMed
-
- Gibson P.G., McDonald V.M. Asthma-COPD overlap 2015: now we are six. Thorax. 2015;70:683–691. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
