

Does heart rate variability correlate with long-term prognosis in myocardial infarction patients treated by early revascularization?
- PMID: 28163834
- PMCID: PMC5253192
- DOI: 10.4330/wjc.v9.i1.27
Does heart rate variability correlate with long-term prognosis in myocardial infarction patients treated by early revascularization?
Abstract
Aim: To assess the prevalence of depressed heart rate variability (HRV) after an acute myocardial infarction (MI), and to evaluate its prognostic significance in the present era of immediate reperfusion.
Methods: Time-domain HRV (obtained from 24-h Holter recordings) was assessed in 326 patients (63.5 ± 12.1 years old; 80% males), two weeks after a complicated MI treated by early reperfusion: 208 ST-elevation myocardial infarction (STEMI) patients (in which reperfusion was successfully obtained within 6 h of symptoms in 94% of cases) and 118 non-ST-elevation myocardial infarction (NSTEMI) patients (percutaneous coronary intervention was performed within 24 h and successful in 73% of cases). Follow-up of the patients was performed via telephone interviews a median of 25 mo after the index event (95%CI of the mean 23.3-28.0). Primary end-point was occurrence of all-cause or cardiac death; secondary end-point was occurrence of major clinical events (MCE, defined as mortality or readmission for new MI, new revascularization, episodes of heart failure or stroke). Possible correlations between HRV parameters (mainly the standard deviation of all normal RR intervals, SDNN), clinical features (age, sex, type of MI, history of diabetes, left ventricle ejection fraction), angiographic characteristics (number of coronary arteries with critical stenoses, success and completeness of revascularization) and long-term outcomes were analysed.
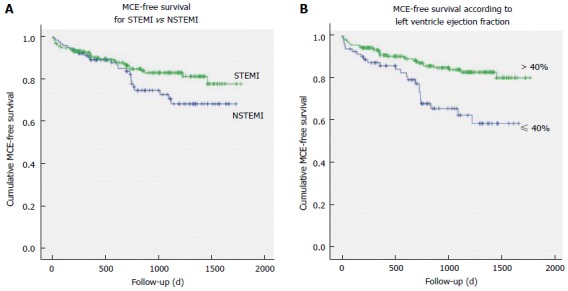
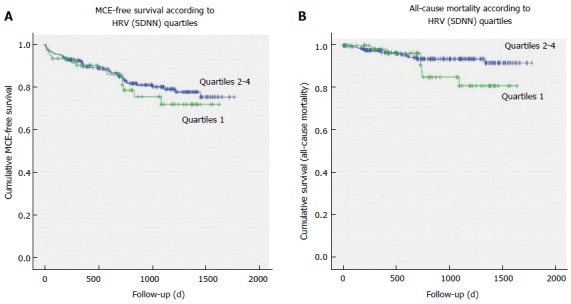
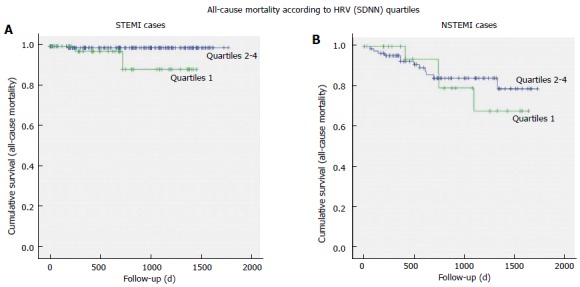
Results: Markedly depressed HRV parameters were present in a relatively small percentage of patients: SDNN < 70 ms was found in 16% and SDNN < 50 ms in 4% of cases. No significant differences were present between STEMI and NSTEMI cases as regards to their distribution among quartiles of SDNN (χ2 =1.536, P = 0.674). Female sex and history of diabetes maintained a significant correlation with lower values of SDNN at multivariate Cox regression analysis (respectively: P = 0.008 and P = 0.008), while no correlation was found between depressed SDNN and history of previous MI (P = 0.999) or number of diseased coronary arteries (P = 0.428) or unsuccessful percutaneous coronary intervention (PCI) (P = 0.691). Patients with left ventricle ejection fraction (LVEF) < 40% presented more often SDNN values in the lowest quartile (P < 0.001). After > 2 years from infarction, a total of 10 patients (3.1%) were lost to follow-up. Overall incidence of MCE at follow-up was similar between STEMI and NSTEMI (P = 0.141), although all-cause and cardiac mortality were higher among NSTEMI cases (respectively: 14% vs 2%, P = 0.001; and 10% vs 1.5%, P = 0.001). The Kaplan-Meier survival curves for all-cause mortality and for cardiac deaths did not reveal significant differences between patients with SDNN in the lowest quartile and other quartiles of SDNN (respectively: P = 0.137 and P = 0.527). Also the MCE-free survival curves were similar between the group of patients with SDNN in the lowest quartile vs the patients of the other SDNN quartiles (P = 0.540), with no difference for STEMI (P = 0.180) or NSTEMI patients (P = 0.541). By the contrary, events-free survival was worse if patients presented with LVEF < 40% (P = 0.001).
Conclusion: In our group of patients with a recent complicated MI, abnormal autonomic parameters have been found with a prevalence that was similar for STEMI and NSTEMI cases, and substantially unchanged in comparison to what reported in the pre-primary-PCI era. Long-term outcomes did not correlate with level of depression of HRV parameters recorded in the subacute phase of the disease, both in STEMI and in NSTEMI patients. These results support lack of prognostic significance of traditional HRV parameters when immediate coronary reperfusion is utilised.
Keywords: Autonomic nervous system; Heart rate variability; Left ventricle ejection fraction; Long-term prognosis; Myocardial infarction; Non-ST-elevation myocardial infarction; Primary percutaneous coronary intervention; ST-elevation myocardial infarction.
Conflict of interest statement
Conflict-of-interest statement: No author has any conflict of interest to declare.
Figures
Similar articles
-
Functional parameters but not heart rate variability correlate with long-term outcomes in St-elevation myocardial infarction patients treated by primary angioplasty.Int J Cardiol. 2016 Dec 1;224:473-481. doi: 10.1016/j.ijcard.2016.09.070. Epub 2016 Sep 23. Int J Cardiol. 2016. PMID: 27736721
-
Prognostic value of heart rate variability after acute myocardial infarction in the era of immediate reperfusion.Herzschrittmacherther Elektrophysiol. 2008 Dec;19(4):161-8. doi: 10.1007/s00399-008-0024-3. Epub 2009 Feb 11. Herzschrittmacherther Elektrophysiol. 2008. PMID: 19214416 Clinical Trial.
-
Impact of renin-angiotensin system inhibitors on long-term clinical outcomes in patients with acute myocardial infarction treated with successful percutaneous coronary intervention with drug-eluting stents: Comparison between STEMI and NSTEMI.Atherosclerosis. 2019 Jan;280:166-173. doi: 10.1016/j.atherosclerosis.2018.11.030. Epub 2018 Nov 27. Atherosclerosis. 2019. PMID: 30529829
-
Contemporary NSTEMI management: the role of the hospitalist.Hosp Pract (1995). 2020 Feb;48(1):1-11. doi: 10.1080/21548331.2020.1701329. Epub 2020 Feb 20. Hosp Pract (1995). 2020. PMID: 31815570 Review.
-
Gender differences in the outcome of cardiac interventions.Herz. 2005 Aug;30(5):375-89. doi: 10.1007/s00059-005-2716-3. Herz. 2005. PMID: 16132240 Review. English, German.
Cited by
-
Evolution of Heart Rate Variability and Heart Rate Turbulence in Patients with Depressive Illness Treated with Selective Serotonin Reuptake Inhibitors.Medicina (Kaunas). 2020 Nov 5;56(11):590. doi: 10.3390/medicina56110590. Medicina (Kaunas). 2020. PMID: 33167574 Free PMC article.
-
B-type natriuretic peptide trumps other prognostic markers in patients assessed for coronary disease.BMC Med. 2019 Apr 3;17(1):72. doi: 10.1186/s12916-019-1306-9. BMC Med. 2019. PMID: 30943979 Free PMC article. Clinical Trial.
-
Renal denervation improves cardiac function by attenuating myocardiocyte apoptosis in dogs after myocardial infarction.BMC Cardiovasc Disord. 2018 May 8;18(1):86. doi: 10.1186/s12872-018-0828-y. BMC Cardiovasc Disord. 2018. PMID: 29739333 Free PMC article.
-
A Comparison Between Culprit Versus Complete Revascularization in Diabetic Patients With Acute Myocardial Infarction.Clin Cardiol. 2024 Nov;47(11):e70046. doi: 10.1002/clc.70046. Clin Cardiol. 2024. PMID: 39540303 Free PMC article.
-
Impact of Short-Term Heart Rate Variability in Patients with STEMI Treated by Delayed versus Immediate Stent in Primary Percutaneous Coronary Intervention: A Prospective Cohort Study.Comput Math Methods Med. 2022 Jun 20;2022:2533664. doi: 10.1155/2022/2533664. eCollection 2022. Comput Math Methods Med. 2022. PMID: 35770121 Free PMC article.
References
-
- Kleiger RE, Miller JP, Bigger JT, Moss AJ. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol. 1987;59:256–262. - PubMed
-
- Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J. 1996;17:354–381. - PubMed
-
- Buccelletti E, Gilardi E, Scaini E, Galiuto L, Persiani R, Biondi A, Basile F, Silveri NG. Heart rate variability and myocardial infarction: systematic literature review and metanalysis. Eur Rev Med Pharmacol Sci. 2009;13:299–307. - PubMed
-
- La Rovere MT, Bigger JT, Marcus FI, Mortara A, Schwartz PJ. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet. 1998;351:478–484. - PubMed
-
- Zuanetti G, Neilson JM, Latini R, Santoro E, Maggioni AP, Ewing DJ. Prognostic significance of heart rate variability in post-myocardial infarction patients in the fibrinolytic era. The GISSI-2 results. Gruppo Italiano per lo Studio della Sopravvivenza nell’ Infarto Miocardico. Circulation. 1996;94:432–436. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
