

Nonpharmacological Interventions Targeted at Delirium Risk Factors, Delivered by Trained Volunteers (Medical and Psychology Students), Reduced Need for Antipsychotic Medications and the Length of Hospital Stay in Aged Patients Admitted to an Acute Internal Medicine Ward: Pilot Study
- PMID: 28164113
- PMCID: PMC5259647
- DOI: 10.1155/2017/1297164
Nonpharmacological Interventions Targeted at Delirium Risk Factors, Delivered by Trained Volunteers (Medical and Psychology Students), Reduced Need for Antipsychotic Medications and the Length of Hospital Stay in Aged Patients Admitted to an Acute Internal Medicine Ward: Pilot Study
Abstract
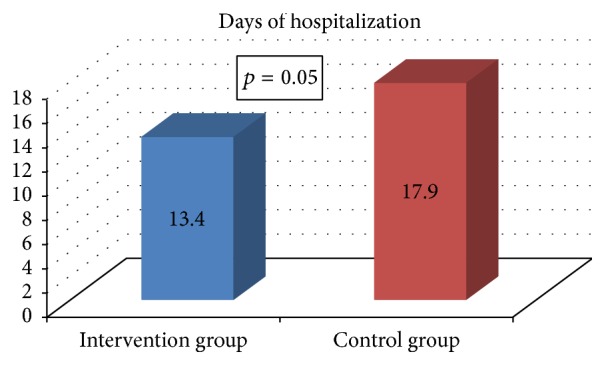
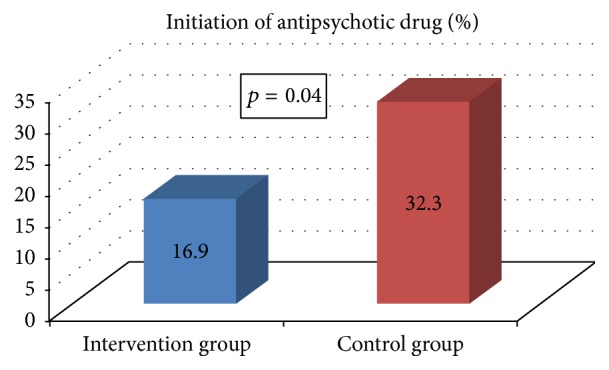
Purpose. Effectiveness of nonpharmacological multicomponent prevention delivered by trained volunteers (medical and psychology students), targeted at delirium risk factors in geriatric inpatients, was assessed at an internal medicine ward in Poland. Patients and Methods. Participants were recruited to intervention and control groups at the internal medicine ward (inclusion criteria: age ≥ 75, acute medical condition, basic orientation, and logical contact on admission; exclusion criteria: life expectancy < 24 hours, surgical hospitalization, isolation due to infectious disease, and discharge to other medical wards). Every day trained volunteers delivered a multicomponent standardized intervention targeted at risk factors of in-hospital complications to the intervention group. The control group, selected using a retrospective individual matching strategy (1 : 1 ratio, regarding age, gender, and time of hospitalization), received standard care. Outcome Measures. Hospitalization time, deaths, falls, delirium episodes, and antipsychotic prescriptions were assessed retrospectively from medical documentation. Results. 130 patients (38.4% males) participated in the study, with 65 in the intervention group. Antipsychotic medications were initiated less frequently in the intervention group compared to the control group. There was a trend towards a shorter hospitalization time and a not statistically significant decrease in deaths in the intervention group. Conclusion. Nonpharmacological multicomponent intervention targeted at delirium risk factors effectively reduced length of hospitalization and need for initiating antipsychotic treatment in elderly patients at the internal medicine ward.
Conflict of interest statement
The authors report no conflict of interests in this work.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
