

Offspring birthweight by gestational age and parental cardiovascular mortality: a population-based cohort study
- PMID: 28165208
- PMCID: PMC5821431
- DOI: 10.1111/1471-0528.14522
Offspring birthweight by gestational age and parental cardiovascular mortality: a population-based cohort study
Abstract
Objective: To estimate risk of parental cardiovascular disease mortality by offspring birthweight.
Design: Population-based cohort study.
Setting and population: Norwegian mothers and fathers with singleton births during 1967-2002 were followed until 2009 by linkage to the Norwegian cause of death registry.
Methods: Hazard ratios by offspring absolute birthweight in grams and birthweight adjusted for gestational age (z-score) were calculated using Cox regression and adjusted for parental age at delivery and year of first birth. Stratified analyses on preterm and term births were performed.
Main outcome measures: Maternal and paternal cardiovascular mortality.
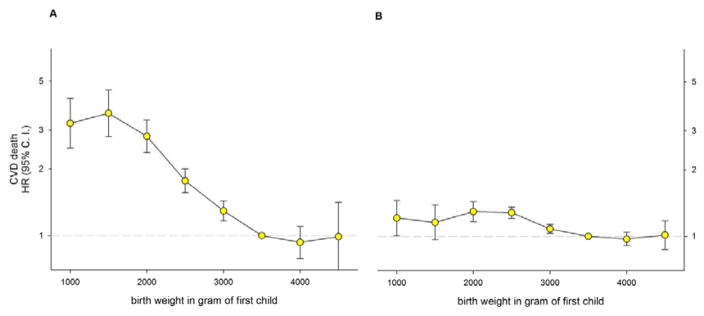
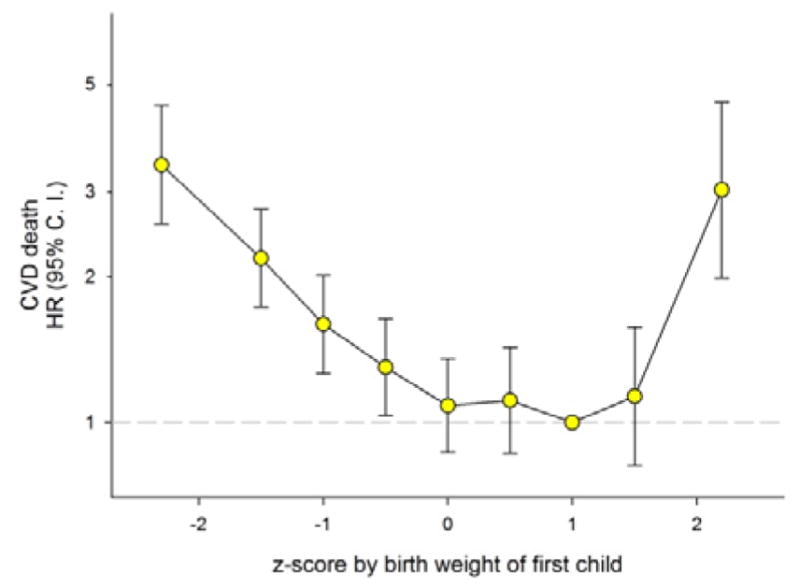
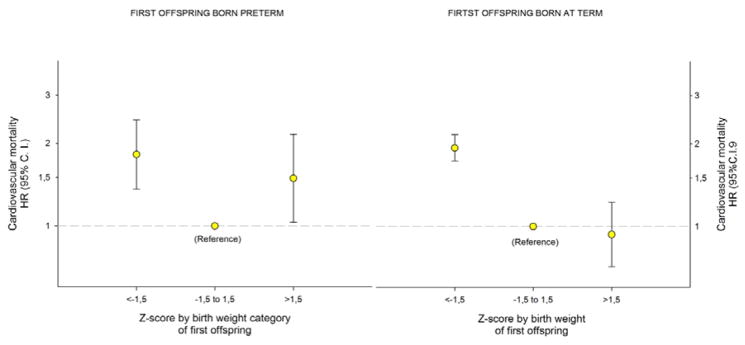
Results: We followed 711 726 mothers and 700 212 fathers and found a strong link between maternal cardiovascular mortality and offspring birthweight but only slight evidence of associations in fathers. Adjusting birthweight for gestational age (by z-score) uncovered an unexpected strong association of large birthweight (z-score > 2.5) with mothers' cardiovascular mortality (hazard ratio 3.0, 95% CI 2.0-4.6). This risk was apparently restricted to preterm births. In stratified analyses (preterm and term births) hazard ratios for maternal cardiovascular mortality were 1.5 (1.03-2.2) for large preterm babies and 0.9 (0.7-1.2) for large term babies (P-value for interaction = 0.02), using normal weight preterm and term, respectively, as references.
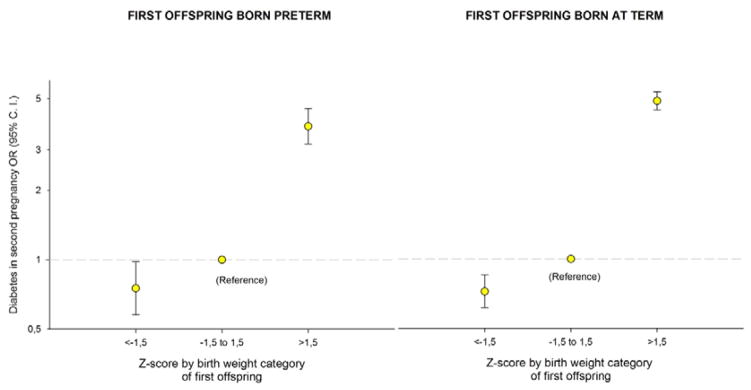
Conclusion: Women having large preterm babies are at increased risk of both diabetes and cardiovascular mortality. The birth of a large preterm baby should increase clinical vigilance for onset of diabetes and other cardiovascular disease risk factors.
Tweetable abstract: Birth of a large preterm baby should increase vigilance for cardiovascular-disease risk factors.
Keywords: Cardiovascular mortality; diabetes; offspring birthweight.
© 2017 Royal College of Obstetricians and Gynaecologists.
Conflict of interest statement
Figures
Comment in
-
Fetal growth and parental cardiovascular risk: preterm birth matters.BJOG. 2018 Feb;125(3):342. doi: 10.1111/1471-0528.14558. Epub 2017 Mar 3. BJOG. 2018. PMID: 28075545 No abstract available.
-
Mothers who give birth to offspring with low birth weight may have increased risk for cardiovascular death.BMJ Evid Based Med. 2019 Feb;24(1):39-40. doi: 10.1136/bmjebm-2018-110987. Epub 2018 Jul 24. BMJ Evid Based Med. 2019. PMID: 30042211 No abstract available.
Similar articles
-
Birthweight in offspring and cardiovascular mortality in their parents, aunts and uncles: a family-based cohort study of 1.35 million births.Int J Epidemiol. 2020 Feb 1;49(1):205-215. doi: 10.1093/ije/dyz156. Int J Epidemiol. 2020. PMID: 31325357 Free PMC article.
-
Mothers' and fathers' birth characteristics and perinatal mortality in their offspring: a population-based cohort study.Paediatr Perinat Epidemiol. 2010 May;24(3):282-92. doi: 10.1111/j.1365-3016.2010.01106.x. Paediatr Perinat Epidemiol. 2010. PMID: 20415758
-
Cardiovascular mortality after pre-eclampsia in one child mothers: prospective, population based cohort study.BMJ. 2012 Nov 27;345:e7677. doi: 10.1136/bmj.e7677. BMJ. 2012. PMID: 23186909 Free PMC article.
-
Maternal fetal programming of birthweight among Australian Aboriginal infants: a population-based data linkage study.Lancet Glob Health. 2019 Apr;7(4):e523-e532. doi: 10.1016/S2214-109X(18)30561-8. Epub 2019 Feb 21. Lancet Glob Health. 2019. PMID: 30799143
-
Offspring birth weight and parental mortality: prospective observational study and meta-analysis.Am J Epidemiol. 2007 Jul 15;166(2):160-9. doi: 10.1093/aje/kwm054. Epub 2007 May 7. Am J Epidemiol. 2007. PMID: 17485730 Review.
Cited by
-
A global view of hypertensive disorders and diabetes mellitus during pregnancy.Nat Rev Endocrinol. 2022 Dec;18(12):760-775. doi: 10.1038/s41574-022-00734-y. Epub 2022 Sep 15. Nat Rev Endocrinol. 2022. PMID: 36109676 Free PMC article. Review.
-
The role of cardiovascular risk factors in maternal cardiovascular disease according to offspring birth characteristics in the HUNT study.Sci Rep. 2021 Nov 26;11(1):22981. doi: 10.1038/s41598-021-99478-4. Sci Rep. 2021. PMID: 34837029 Free PMC article.
-
Update on sex specific risk factors in cardiovascular disease.Front Cardiovasc Med. 2024 Feb 6;11:1352675. doi: 10.3389/fcvm.2024.1352675. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38380176 Free PMC article. Review.
-
Pregnancy complications in last pregnancy and mothers' long-term cardiovascular mortality: does the relation differ from that of complications in first pregnancy? A population-based study.BMC Womens Health. 2023 Jul 4;23(1):355. doi: 10.1186/s12905-023-02503-z. BMC Womens Health. 2023. PMID: 37403040 Free PMC article.
-
A Machine Learning-Based Prediction Model for Cardiovascular Risk in Women With Preeclampsia.Front Cardiovasc Med. 2021 Oct 27;8:736491. doi: 10.3389/fcvm.2021.736491. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34778400 Free PMC article.
References
-
- Mosca L, Hammond G, Mochari-Greenberger H, Towfighi A, Albert MA, et al. American Heart Association Cardiovascular D. Fifteen-year trends in awareness of heart disease in women: results of a 2012 American Heart Association national survey. Circulation. 2013 Mar 19;127(11):1254–63. e1–29. - PMC - PubMed
-
- Shaw LJ, Bairey Merz CN, Pepine CJ, Reis SE, Bittner V, Kelsey SF, et al. Insights from the NHLBI-Sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study: Part I: gender differences in traditional and novel risk factors, symptom evaluation, and gender-optimized diagnostic strategies. J Am Coll Cardiol. 2006 Feb 7;47(3 Suppl):S4–S20. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
