

Occlusal stabilization splint for patients with temporomandibular disorders: Meta-analysis of short and long term effects
- PMID: 28166255
- PMCID: PMC5293221
- DOI: 10.1371/journal.pone.0171296
Occlusal stabilization splint for patients with temporomandibular disorders: Meta-analysis of short and long term effects
Abstract
Background: Psychological discomfort, physical disability and functional limitations of the orofacial system have a major impact on everyday life of patients with temporomandibular disorders (TMDs). In this study we sought to determine short and long term effects of stabilization splint (SS) in treatment of TMDs, and to identify factors influencing its efficacy.
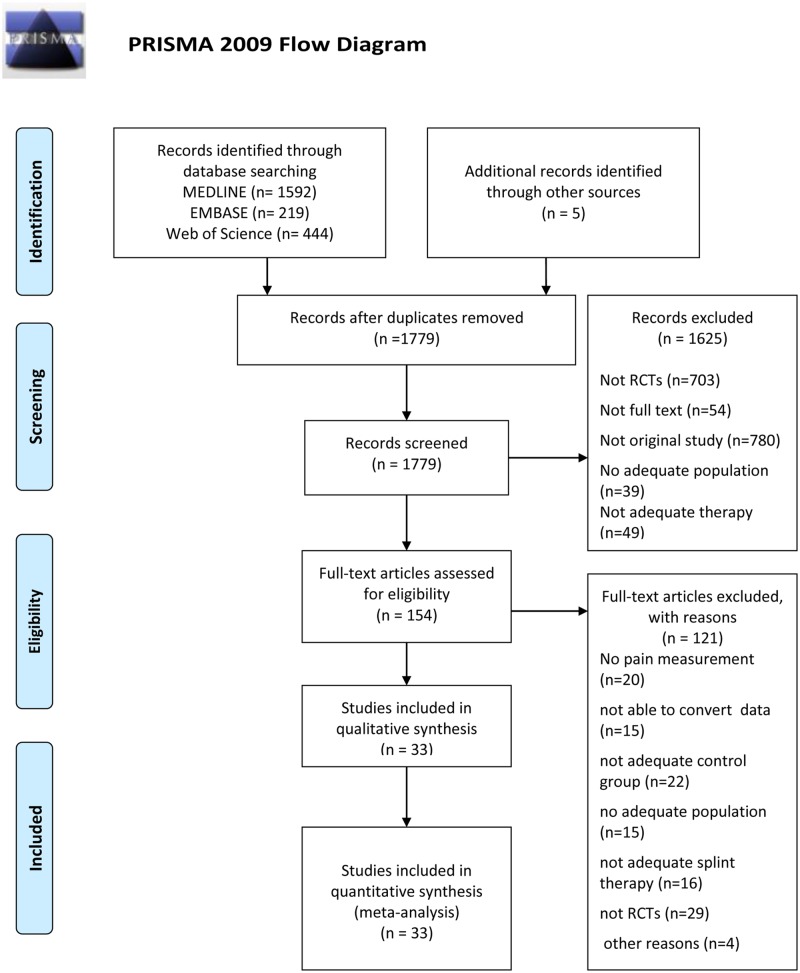
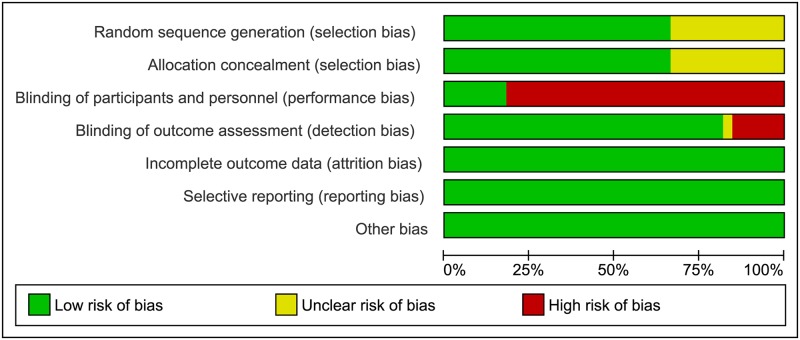
Methods: MEDLINE, Web of Science and EMBASE were searched for randomized controlled trials (RCTs) comparing SS to: non-occluding splint, occlusal oral appliances, physiotherapy, behavioral therapy, counseling and no treatment. Random effects method was used to summarize outcomes. The effect estimates were expressed as odds ratio (OR) or standardized mean difference (SMD) with 95% confidence interval. Subgroup analyses were carried out according to the use of Research Diagnostic Criteria (RDC/TMD) and TMDs origin. Strength of evidence was assessed by GRADE. Meta-regression was applied.
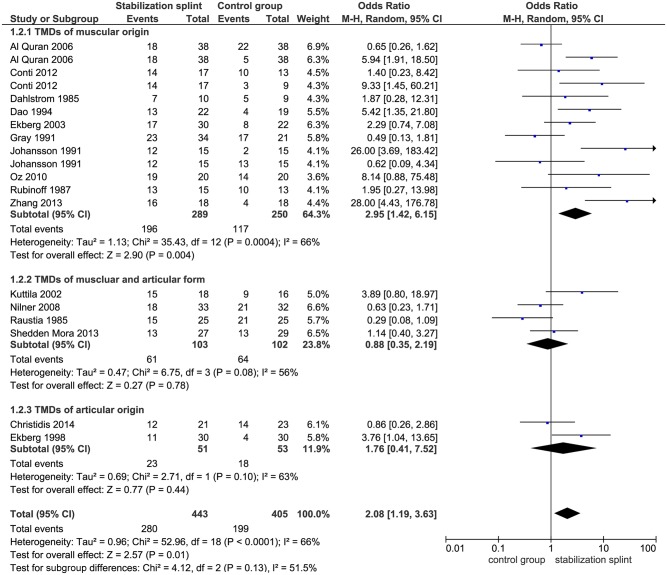
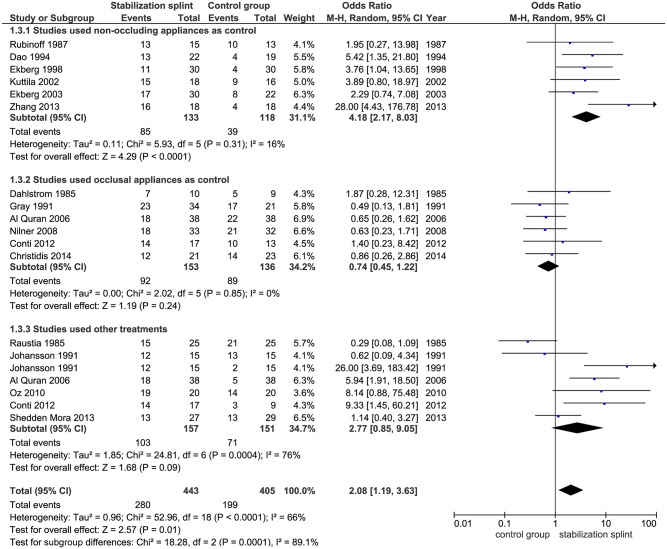
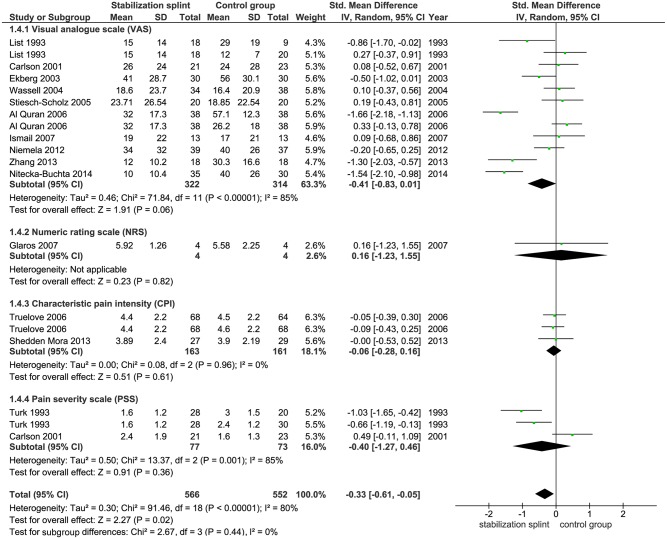
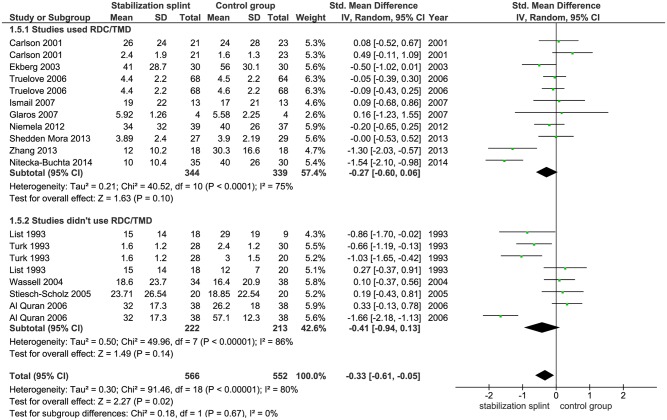
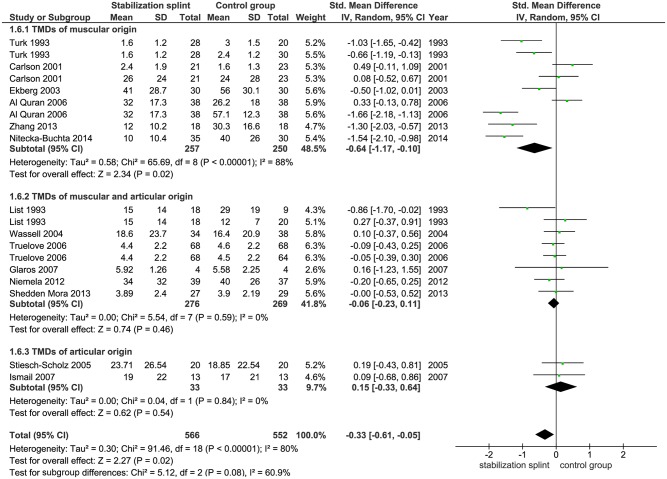
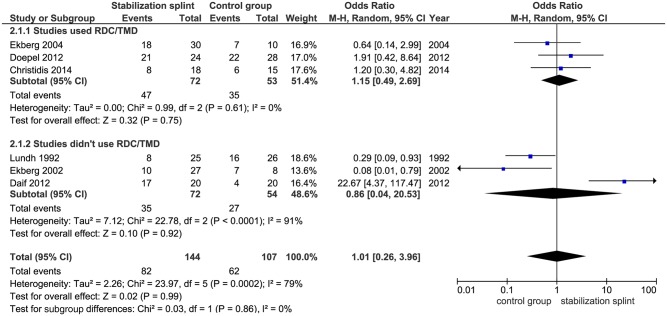
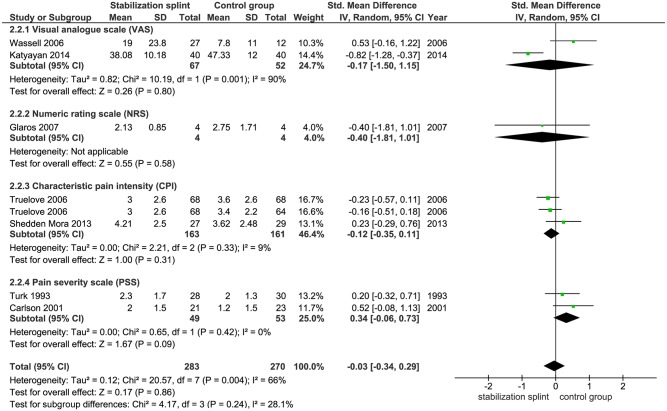
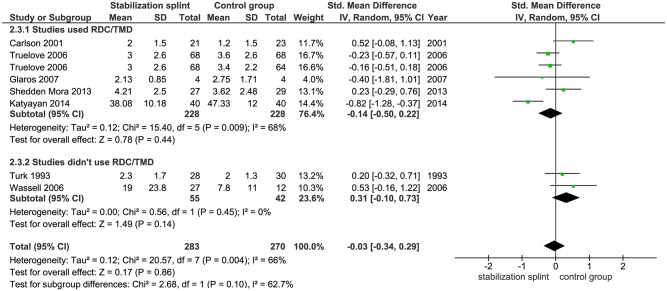
Results: Thirty three eligible RCTs were included in meta-analysis. In short term, SS presented positive overall effect on pain reduction (OR 2.08; p = 0.01) and pain intensity (SMD -0.33; p = 0.02). Subgroup analyses confirmed SS effect in studies used RDC/TMD and revealed its effect in patients with TMDs of muscular origin. Important decrease of muscle tenderness (OR 1.97; p = 0.03) and improvement of mouth opening (SMD -0.30; p = 0.04) were found. SS in comparison to oral appliances showed no difference (OR 0.74; p = 0.24). Meta-regression identified continuous use of SS during the day as a factor influencing efficacy (p = 0.01). Long term results showed no difference in observed outcomes between groups. Low quality of evidence was found for primary outcomes.
Conclusion: SS presented short term benefit for patients with TMDs. In long term follow up, the effect is equalized with other therapeutic modalities. Further studies based on appropriate use of standardized criteria for patient recruitment and outcomes under assessment are needed to better define SS effect persistence in long term.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Roldan-Barraza C, Janko S, Villanueva J, Araya I, Lauer H-C. A Systematic Review and Meta-analysis of Usual Treatment Versus Psychosocial Interventions in the Treatment of Myofascial Temporomandibular Disorder Pain. Journal of Oral & Facial Pain and Headache. 2014;28(3):205–22. - PubMed
-
- Turp JC, Motschall E, Schindler HJ, Heydecke G. In patients with temporomandibular disorders, do particular interventions influence oral health-related quality of life? A qualitative systematic review of the literature. Clin Oral Implants Res. 2007;18 Suppl 3:127–37. Epub 2007/06/28. - PubMed
-
- Macfarlane TV, Glenny AM, Worthington HV. Systematic review of population-based epidemiological studies of oro-facial pain. J Dent. 2001;29(7):451–67. Epub 2002/01/26. - PubMed
-
- Drangsholt M, LeResche L. Temporomandibular disorder pain In: Crombie I, Croft P, Linton S, LeResche L, Von Korff Me, editors. Epidemiology of Pain. Seattle: IASP Press; 1999. p. 203–33.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
