

Associations between chronic comorbidity and exacerbation risk in primary care patients with COPD
- PMID: 28166777
- PMCID: PMC5294875
- DOI: 10.1186/s12931-017-0512-2
Associations between chronic comorbidity and exacerbation risk in primary care patients with COPD
Abstract
Background: COPD often coexists with chronic conditions that may influence disease prognosis. We investigated associations between chronic (co)morbidities and exacerbations in primary care COPD patients.
Method: Retrospective cohort study based on 2012-2013 electronic health records from 179 Dutch general practices. Comorbidities from patients with physician-diagnosed COPD were categorized according to International Classification of Primary Care (ICPC) codes. Chi-squared tests, uni- and multivariable logistic, and Cox regression analyses were used to study associations with exacerbations, defined as oral corticosteroid prescriptions.
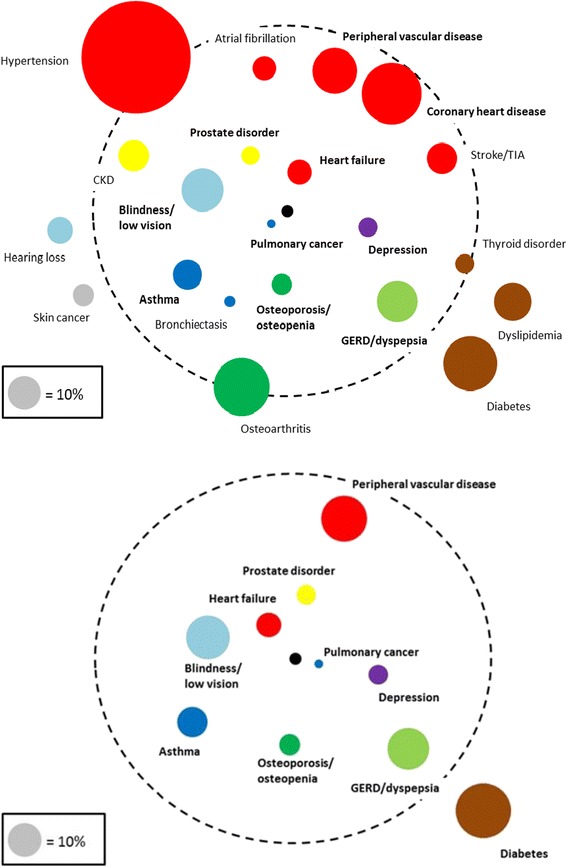
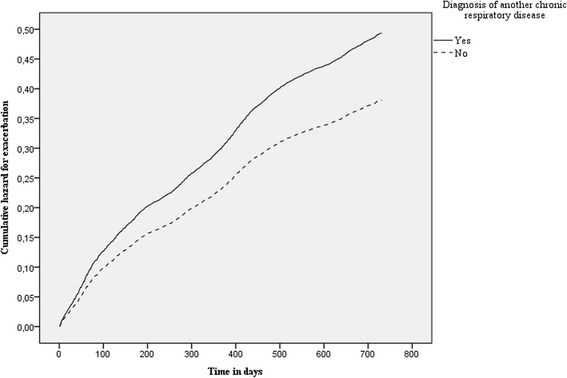
Results: Fourteen thousand six hundred three patients with COPD could be studied (mean age 67 (SD 12) years, 53% male) for two years. At baseline 12,826 (88%) suffered from ≥1 comorbidities, 3263 (22%) from ≥5. The most prevalent comorbidities were hypertension (35%), coronary heart disease (19%), and osteoarthritis (18%). Several comorbidities showed statistically significant associations with frequent (i.e., ≥2/year) exacerbations: heart failure (odds ratio [OR], 95% confidence interval: 1.72; 1.38-2.14), blindness & low vision (OR 1.46; 1.21-1.75), pulmonary cancer (OR 1.85; 1.28-2.67), depression 1.48; 1.14-1.91), prostate disorders (OR 1.50; 1.13-1.98), asthma (OR 1.36; 1.11-1.70), osteoporosis (OR 1.41; 1.11-1.80), diabetes (OR 0.80; 0.66-0.97), dyspepsia (OR 1.25; 1.03-1.50), and peripheral vascular disease (OR 1.20; 1.00-1.45). From all comorbidity categories, having another chronic respiratory disease beside COPD showed the highest risk for developing a new exacerbation (Cox hazard ratio 1.26; 1.17-1.36).
Conclusion: Chronic comorbidities are highly prevalent in primary care COPD patients. Several chronic comorbidities were associated with having frequent exacerbations and increased exacerbation risk.
Figures
References
-
- From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2016. Available from: http://www.goldcopd.org/. Accessed 16 Jan 2017.
-
- Negewo NA, McDonald VM, Gibson PG. Comorbidity in chronic obstructive pulmonary disease. Respir Invest. 2015;53(6):249–58. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
