

Doppler Endoscopic Probe Monitoring of Blood Flow Improves Risk Stratification and Outcomes of Patients With Severe Nonvariceal Upper Gastrointestinal Hemorrhage
- PMID: 28167214
- PMCID: PMC5613762
- DOI: 10.1053/j.gastro.2017.01.042
Doppler Endoscopic Probe Monitoring of Blood Flow Improves Risk Stratification and Outcomes of Patients With Severe Nonvariceal Upper Gastrointestinal Hemorrhage
Abstract
Background & aims: For 4 decades, stigmata of recent hemorrhage in patients with nonvariceal lesions have been used for risk stratification and endoscopic hemostasis. The arterial blood flow that underlies the stigmata rarely is monitored, but can be used to determine risk for rebleeding. We performed a randomized controlled trial to determine whether Doppler endoscopic probe monitoring of blood flow improves risk stratification and outcomes in patients with severe nonvariceal upper gastrointestinal hemorrhage.
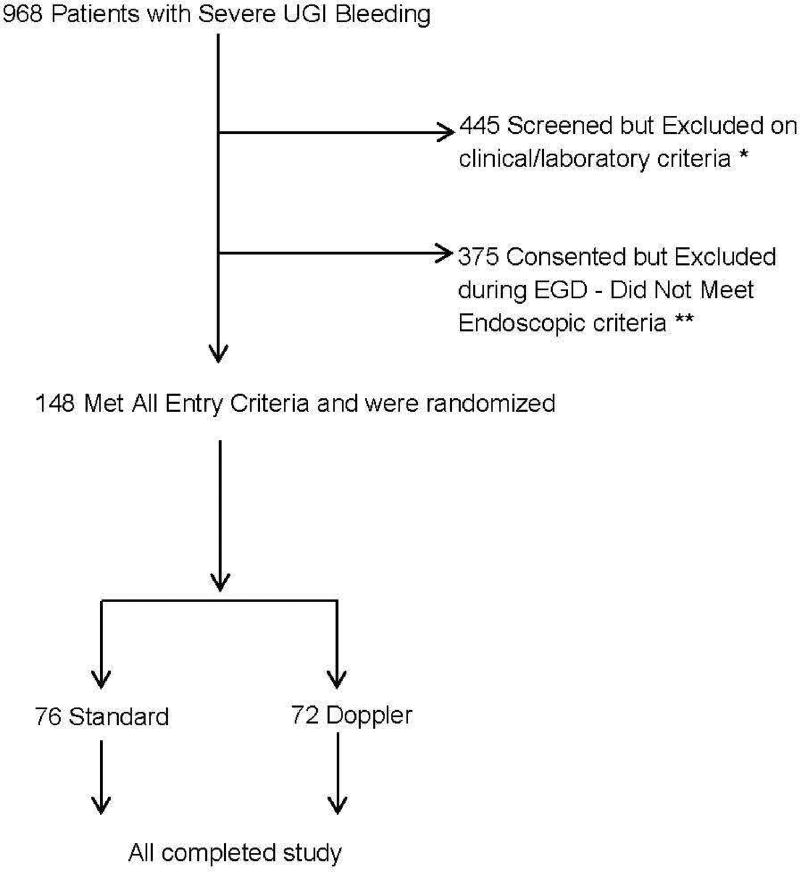
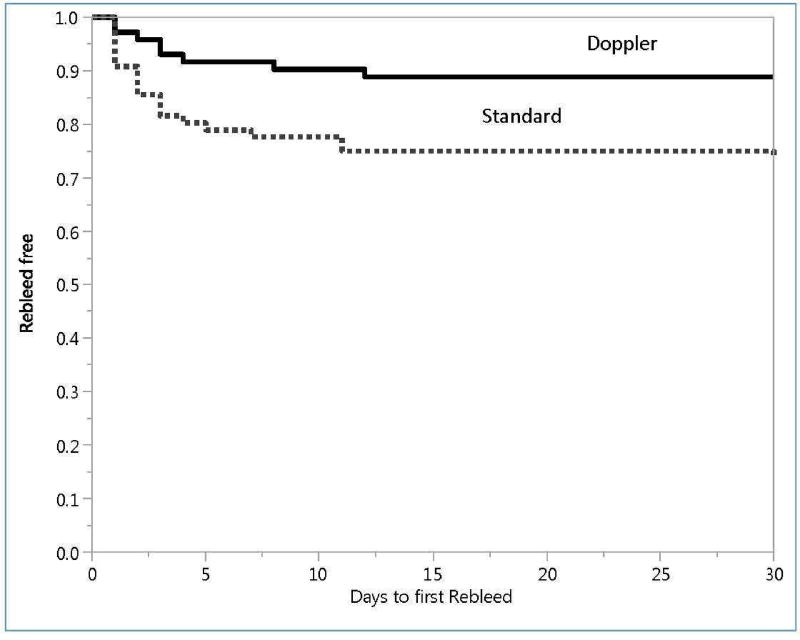
Methods: In a single-blind study performed at 2 referral centers we assigned 148 patients with severe nonvariceal upper gastrointestinal bleeding (125 with ulcers, 19 with Dieulafoy's lesions, and 4 with Mallory Weiss tears) to groups that underwent standard, visually guided endoscopic hemostasis (control, n = 76), or endoscopic hemostasis assisted by Doppler monitoring of blood flow under the stigmata (n = 72). The primary outcome was the rate of rebleeding after 30 days; secondary outcomes were complications, death, and need for transfusions, surgery, or angiography.
Results: There was a significant difference in the rates of lesion rebleeding within 30 days of endoscopic hemostasis in the control group (26.3%) vs the Doppler group (11.1%) (P = .0214). The odds ratio for rebleeding with Doppler monitoring was 0.35 (95% confidence interval, 0.143-0.8565) and the number needed to treat was 7.
Conclusions: In a randomized controlled trial of patients with severe upper gastrointestinal hemorrhage from ulcers or other lesions, Doppler probe guided endoscopic hemostasis significantly reduced 30-day rates of rebleeding compared with standard, visually guided hemostasis. Guidelines for nonvariceal gastrointestinal bleeding should incorporate these results. ClinicalTrials.gov no: NCT00732212 (CLIN-013-07F).
Keywords: Clinical Trial; Endoscopy; Stigmata of Hemorrhage; UGI Bleeding.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Should We All Be Using the Doppler Endoscopic Probe in Nonvariceal Upper Gastrointestinal Bleeding?Gastroenterology. 2017 May;152(6):1280-1282. doi: 10.1053/j.gastro.2017.03.021. Epub 2017 Mar 27. Gastroenterology. 2017. PMID: 28351653 No abstract available.
-
Reply.Gastroenterology. 2017 Sep;153(3):868-869. doi: 10.1053/j.gastro.2017.08.002. Epub 2017 Aug 3. Gastroenterology. 2017. PMID: 28781222 No abstract available.
References
-
- Storey DW, Bown SG, Swain CP, Salmon PR, Kirkham JS, Northfield TC. Endoscopic prediction of recurrent bleeding in peptic ulcers. N Engl J Med. 1981;305:915–6. - PubMed
-
- Swain CP, Storey DW, Bown SG, et al. Nature of bleeding vessel in recurrently bleeding gastric ulcers. Gastroenterology. 1986;90:595–608. - PubMed
-
- Johnston JH. The sentinel clot and invisible vessel: pathologic anatomy of bleeding peptic ulcer. Gastrointest Endosc. 1984;30:313–15. - PubMed
-
- Swain P. Perception and interpretation: The problem of the visible vessel. Endoscopy. 1998;30:570–74. - PubMed
-
- Forrest JA, Finlayson ND, Shearman DJ. Endoscopy in gastrointestinal bleeding. Lancet. 1974;2:394–7. - PubMed
