

Removal of all ovarian tissue versus conserving ovarian tissue at time of hysterectomy in premenopausal patients with benign disease: study using routine data and data linkage
- PMID: 28167486
- PMCID: PMC5421461
- DOI: 10.1136/bmj.j372
Removal of all ovarian tissue versus conserving ovarian tissue at time of hysterectomy in premenopausal patients with benign disease: study using routine data and data linkage
Abstract
Objective: To conduct a nationwide study of associations between removal of all ovarian tissue versus conservation of at least one ovary at the time of hysterectomy and important health outcomes (ischaemic heart disease, cancer, and all cause mortality).
Study design and setting: Retrospective analysis of the English Hospital Episode Statistics database linked to national registers of deprivation indices and of deaths.
Participants: 113 679 patients aged 35-45 who had had a hysterectomy for benign conditions between April 2004 and March 2014.
Exposures: Bilateral ovarian removal versus no removal or unilateral ovarian removal (ovarian conservation).
Main outcome measures: Hospital admissions for ischaemic heart disease, cancer, or attempted suicide; deaths, overall and from heart disease, cancer, or suicide. Statistical adjustments were made using Cox regression and propensity score matching for potential confounders.
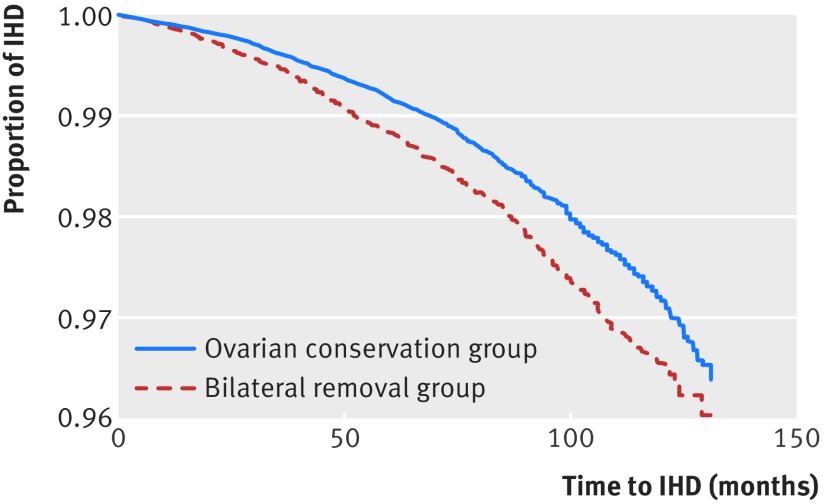
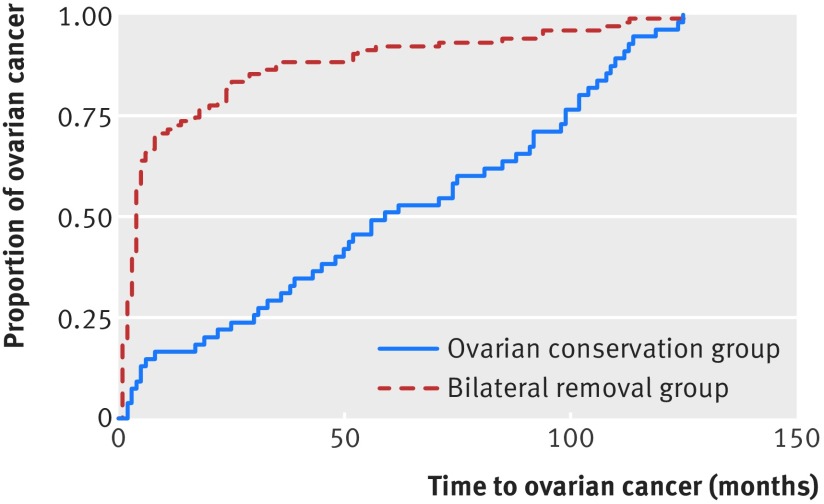
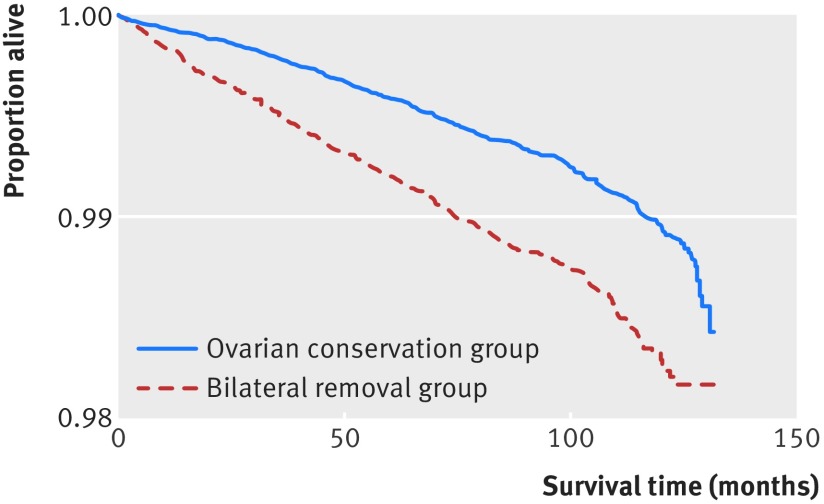
Results: A third of patients had bilateral ovarian removal. Patients in the ovarian conservation group were less likely to be admitted for ischaemic heart disease after hysterectomy than were those in the bilateral removal group (adjusted hazard ratio 0.85, 95% confidence interval 0.77 to 0.93; P=0.001). They were also less likely to have a cancer related post-hysterectomy admission (adjusted hazard ratio 0.83, 0.78 to 0.89; P<0.001). A significant difference in all cause mortality was also seen: 0.60% (456/76 581) of patients with ovarian conservation compared with 1.01% (376/37 098) of patients with bilateral removal. Again, this difference in favour of ovarian conservation was significant (adjusted hazard ratio 0.64, 0.55 to 0.73; P<0.001). Fewer deaths related specifically to heart disease (adjusted hazard ratio 0.50, 0.28 to 0.90; P=0.02) and to cancer (0.54, 0.45 to 0.65; P<0.001) occurred in the ovarian conservation group than in the bilateral removal group. No significant difference between groups was found relating to suicide (attempted or completed). The results after propensity score matching were essentially unchanged.
Conclusion: Patients who had ovarian conservation had a significantly lower hazard of all cause mortality compared with those who had bilateral ovarian removal and also had lower death rates from ischaemic heart disease and cancer. Consistent with this observation, admissions to hospital for both ischaemic heart disease and cancer were also lower in the ovarian conservation group than in the bilateral removal group. Although removal of both ovaries protects against subsequent development of ovarian cancer, premenopausal women should be advised that this benefit comes at the cost of an increased risk of cardiovascular disease and of other (more prevalent) cancers and higher overall mortality.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Parker WH, Broder MS, Chang E, et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the nurses’ health study. Obstet Gynecol 2009;113:1027-37. 10.1097/AOG.0b013e3181a11c64 pmid:19384117. - DOI - PMC - PubMed
-
- Cancer Research UK. Ovarian cancer incidence statistics. 2016. http://www.cancerresearchuk.org/health-professional/cancer-statistics/st....
-
- Parker WH, Feskanich D, Broder MS, et al. Long-term mortality associated with oophorectomy compared with ovarian conservation in the nurses’ health study. Obstet Gynecol 2013;121:709-16. 10.1097/AOG.0b013e3182864350 pmid:23635669. - DOI - PMC - PubMed
-
- McCarthy AM, Menke A, Ouyang P, Visvanathan K. Bilateral oophorectomy, body mass index, and mortality in U.S. women aged 40 years and older. Cancer Prev Res (Phila) 2012;5:847-54. 10.1158/1940-6207.CAPR-11-0430 pmid:22556202. - DOI - PMC - PubMed
-
- Rivera CM, Grossardt BR, Rhodes DJ, et al. Increased cardiovascular mortality after early bilateral oophorectomy. Menopause 2009;16:15-23. 10.1097/gme.0b013e31818888f7 pmid:19034050. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous