

Targeting Bruton tyrosine kinase with ibrutinib in relapsed/refractory marginal zone lymphoma
- PMID: 28167659
- PMCID: PMC5399483
- DOI: 10.1182/blood-2016-10-747345
Targeting Bruton tyrosine kinase with ibrutinib in relapsed/refractory marginal zone lymphoma
Abstract
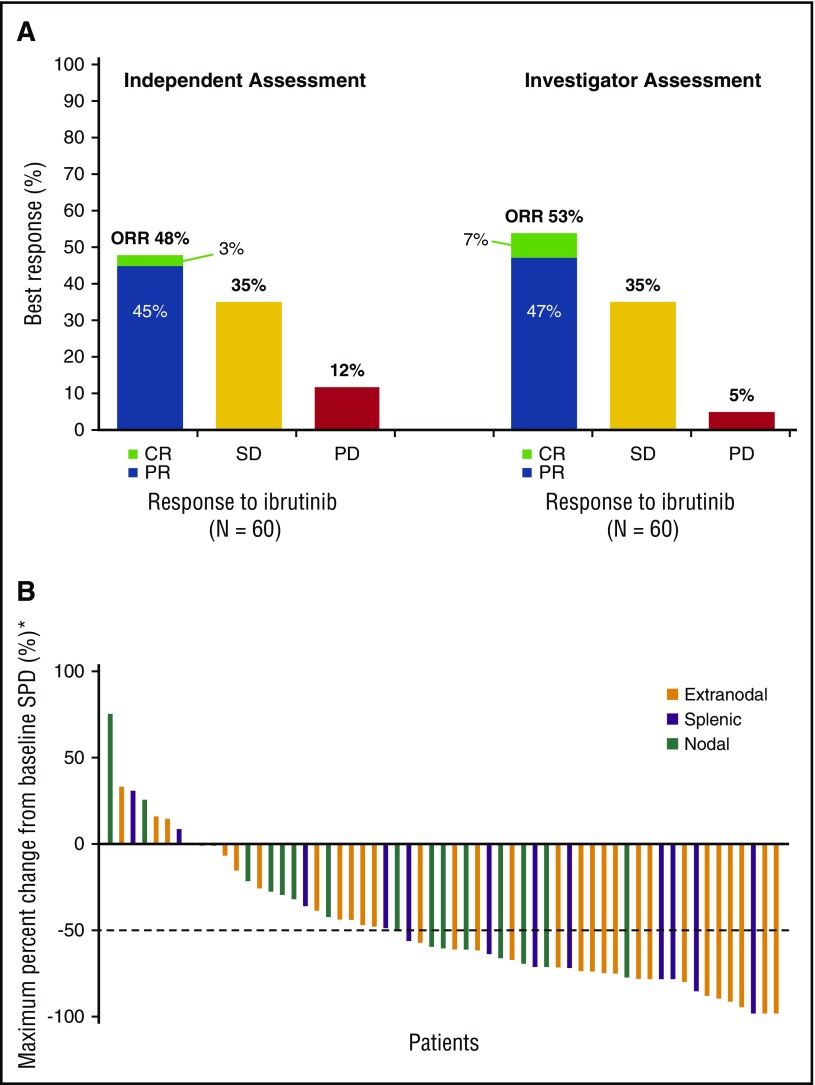
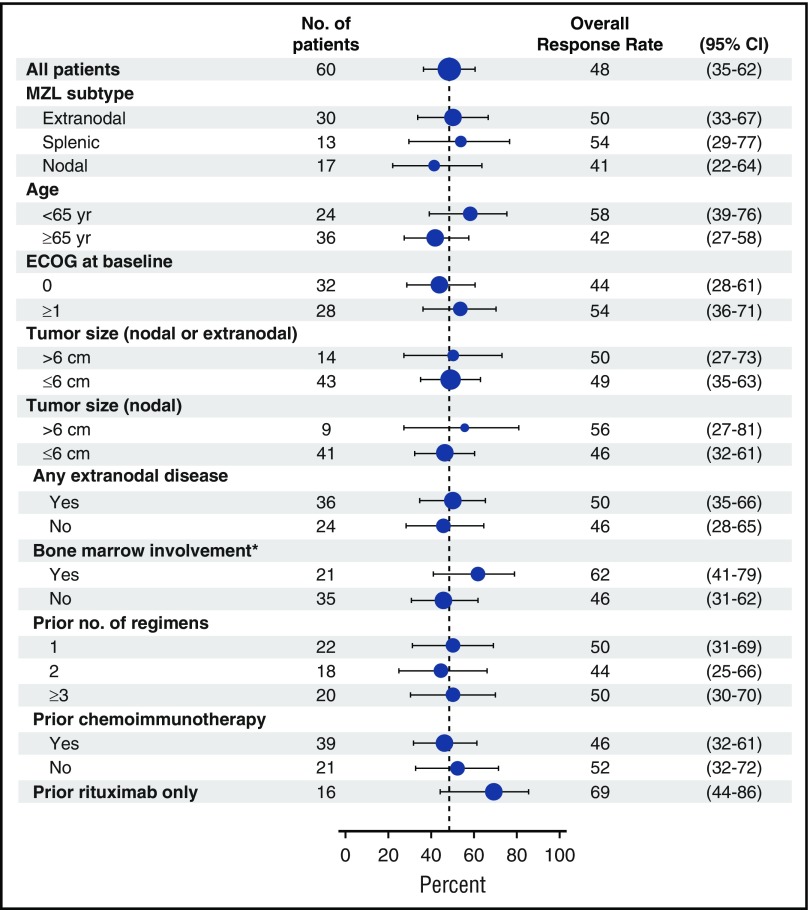
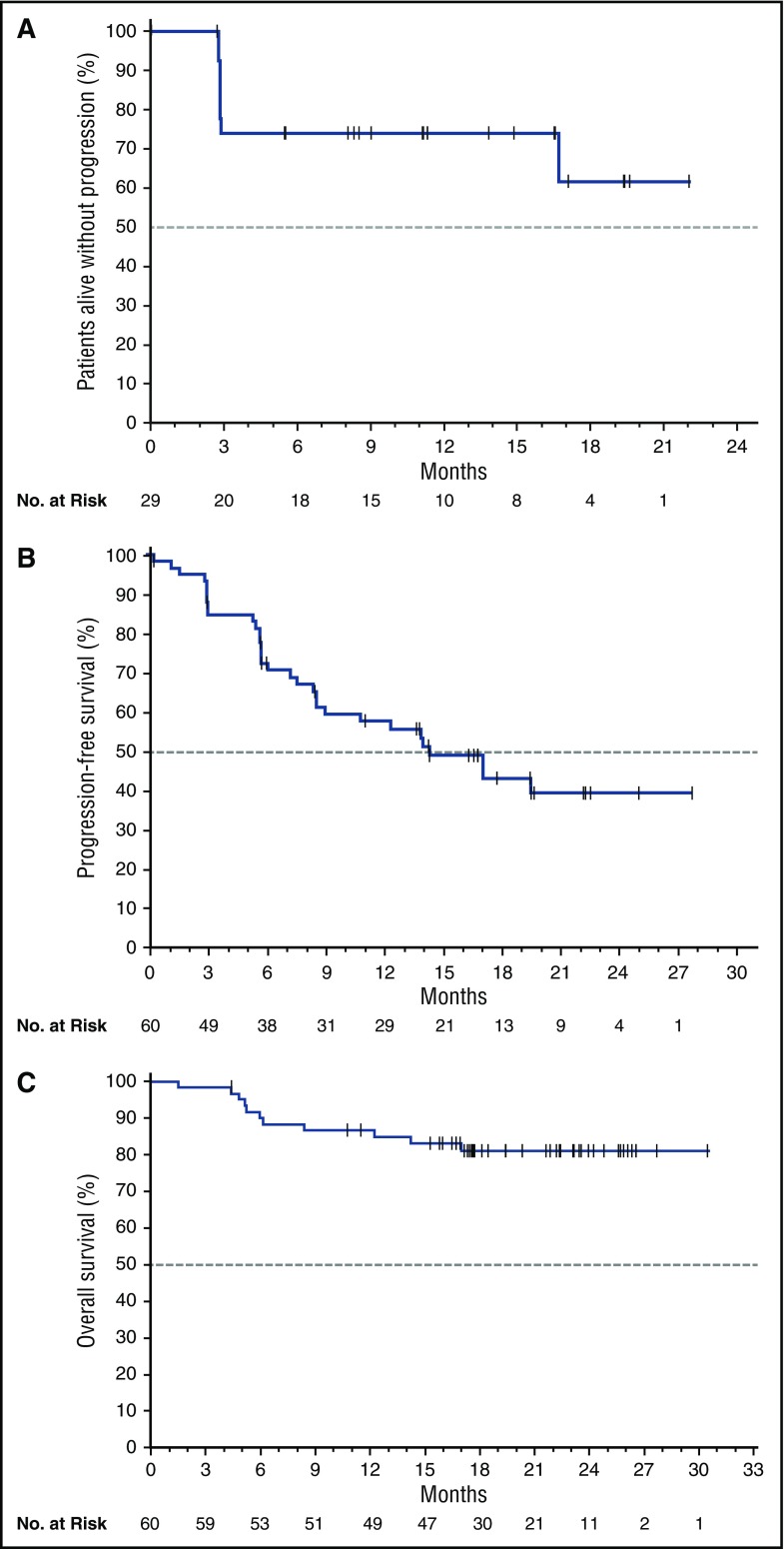
Marginal zone lymphoma (MZL) is a heterogeneous B-cell malignancy for which no standard treatment exists. MZL is frequently linked to chronic infection, which may induce B-cell receptor (BCR) signaling, resulting in aberrant B-cell survival and proliferation. We conducted a multicenter, open-label, phase 2 study to evaluate the efficacy and safety of ibrutinib in previously treated MZL. Patients with histologically confirmed MZL of all subtypes who received ≥1 prior therapy with an anti-CD20 antibody-containing regimen were treated with 560 mg ibrutinib orally once daily until progression or unacceptable toxicity. The primary end point was independent review committee-assessed overall response rate (ORR) by 2007 International Working Group criteria. Among 63 enrolled patients, median age was 66 years (range, 30-92). Median number of prior systemic therapies was 2 (range, 1-9), and 63% received ≥1 prior chemoimmunotherapy. In 60 evaluable patients, ORR was 48% (95% confidence interval [CI], 35-62). With median follow-up of 19.4 months, median duration of response was not reached (95% CI, 16.7 to not estimable), and median progression-free survival was 14.2 months (95% CI, 8.3 to not estimable). Grade ≥3 adverse events (AEs; >5%) included anemia, pneumonia, and fatigue. Serious AEs of any grade occurred in 44%, with grade 3-4 pneumonia being the most common (8%). Rates of discontinuation and dose reductions due to AEs were 17% and 10%, respectively. Single-agent ibrutinib induced durable responses with a favorable benefit-risk profile in patients with previously treated MZL, confirming the role of BCR signaling in this malignancy. As the only approved therapy, ibrutinib provides a treatment option without chemotherapy for MZL. This study is registered at www.clinicaltrials.gov as #NCT01980628.
© 2017 by The American Society of Hematology.
Figures
Comment in
-
Targeted therapies: Ibrutinib: new option for relapsed MZL.Nat Rev Clin Oncol. 2017 Mar 20;14(4):200. doi: 10.1038/nrclinonc.2017.26. Nat Rev Clin Oncol. 2017. PMID: 28316331 No abstract available.
-
Efficacy in the margins of NHL with ibrutinib.Blood. 2017 Apr 20;129(16):2207-2208. doi: 10.1182/blood-2017-02-769042. Blood. 2017. PMID: 28428233 No abstract available.
References
-
- Swerdlow SH, Campo E, Harris NL, et al., eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed Lyon, France: IARC Press; 2008.
-
- A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. The Non-Hodgkin’s Lymphoma Classification Project. Blood. 1997;89(11):3909-3918. - PubMed
-
- Al-Hamadani M, Habermann TM, Cerhan JR, Macon WR, Maurer MJ, Go RS. Non-Hodgkin lymphoma subtype distribution, geodemographic patterns, and survival in the US: A longitudinal analysis of the National Cancer Data Base from 1998 to 2011. Am J Hematol. 2015;90(9):790-795. - PubMed
-
- Cervetti G, Galimberti S, Sordi E, et al. Significant efficacy of 2-CdA with or without rituximab in the treatment of splenic marginal zone lymphoma (SMZL). Ann Oncol. 2010;21(4):851-854. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
