

Prediction of Preeclampsia Using the Soluble fms-Like Tyrosine Kinase 1 to Placental Growth Factor Ratio: A Prospective Cohort Study of Unselected Nulliparous Women
- PMID: 28167687
- PMCID: PMC5344177
- DOI: 10.1161/HYPERTENSIONAHA.116.08620
Prediction of Preeclampsia Using the Soluble fms-Like Tyrosine Kinase 1 to Placental Growth Factor Ratio: A Prospective Cohort Study of Unselected Nulliparous Women
Abstract
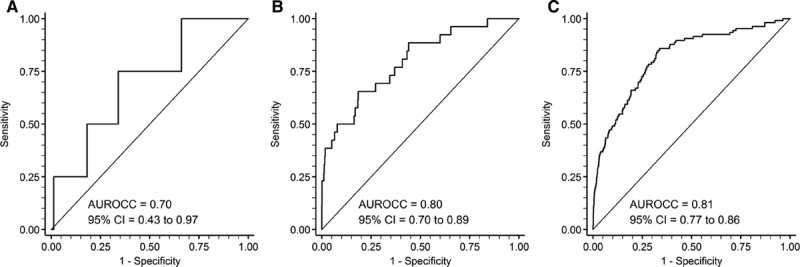
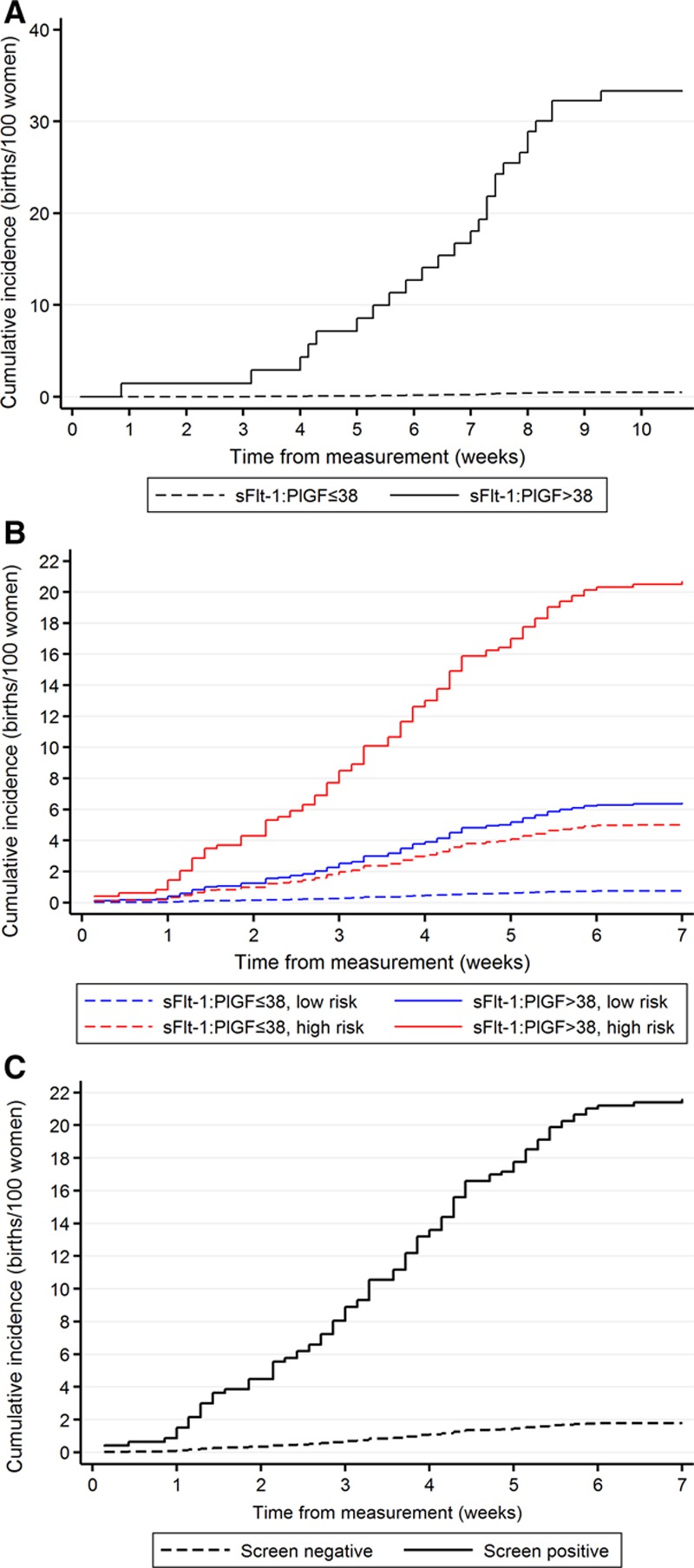
We sought to assess the ratio of sFlt-1 (soluble fms-like tyrosine kinase 1) to PlGF (placental growth factor) in maternal serum as a screening test for preeclampsia in unselected nulliparous women with a singleton pregnancy. We studied 4099 women recruited to the POP study (Pregnancy Outcome Prediction) (Cambridge, United Kingdom). The sFlt-1:PlGF ratio was measured using the Roche Cobas e411 platform at ≈20, ≈28, and ≈36 weeks of gestational age (wkGA). Screen positive was defined as an sFlt-1:PlGF ratio >38, but higher thresholds were also studied. At 28 wkGA, an sFlt-1:PlGF ratio >38 had a positive predictive value (PPV) of 32% for preeclampsia and preterm birth, and the PPV was similar comparing women with low and high prior risk of disease. At 36 wkGA, an sFlt-1:PlGF ratio >38 had a PPV for severe preeclampsia of 20% in high-risk women and 6.4% in low-risk women. At 36 wkGA, an sFlt-1:PlGF ratio >110 had a PPV of 30% for severe preeclampsia, and the PPV was similar comparing low- and high-risk women. Overall, at 36 wkGA, 195 (5.2%) women either had an sFlt-1:PlGF ratio of >110 or an sFlt-1:PlGF ratio >38 plus maternal risk factors: 43% of these women developed preeclampsia, about half with severe features. Among low-risk women at 36 wkGA, an sFlt-1:PlGF ratio ≤38 had a negative predictive value for severe preeclampsia of 99.2%. The sFlt-1:PlGF ratio provided clinically useful prediction of the risk of the most important manifestations of preeclampsia in a cohort of unselected nulliparous women.
Keywords: clinical markers; cohort studies; immunoassay; pregnancy; risk factors.
© 2017 The Authors.
Figures
Comment in
-
Angiogenic Markers in Transition: Thinking Positive.Hypertension. 2017 Apr;69(4):578-579. doi: 10.1161/HYPERTENSIONAHA.116.08739. Epub 2017 Feb 6. Hypertension. 2017. PMID: 28167684 No abstract available.
References
-
- Lyall F, Belfort M. Pre-Eclampsia: Etiology and Clinical Practice. Cambridge, United Kingdom: Cambridge University Press; 2007.
-
- Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, Schisterman EF, Thadhani R, Sachs BP, Epstein FH, Sibai BM, Sukhatme VP, Karumanchi SA. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004;350:672–683. doi: 10.1056/NEJMoa031884. - PubMed
-
- Levine RJ, Lam C, Qian C, Yu KF, Maynard SE, Sachs BP, Sibai BM, Epstein FH, Romero R, Thadhani R, Karumanchi SA CPEP Study Group. Soluble endoglin and other circulating antiangiogenic factors in preeclampsia. N Engl J Med. 2006;355:992–1005. doi: 10.1056/NEJMoa055352. - PubMed
-
- Zeisler H, Llurba E, Chantraine F, Vatish M, Staff AC, Sennström M, Olovsson M, Brennecke SP, Stepan H, Allegranza D, Dilba P, Schoedl M, Hund M, Verlohren S. Predictive value of the sFlt-1:PlGF ratio in women with suspected preeclampsia. N Engl J Med. 2016;374:13–22. doi: 10.1056/NEJMoa1414838. - PubMed
-
- Verlohren S, Herraiz I, Lapaire O, Schlembach D, Zeisler H, Calda P, Sabria J, Markfeld-Erol F, Galindo A, Schoofs K, Denk B, Stepan H. New gestational phase-specific cutoff values for the use of the soluble fms-like tyrosine kinase-1/placental growth factor ratio as a diagnostic test for preeclampsia. Hypertension. 2014;63:346–352. doi: 10.1161/HYPERTENSIONAHA.113.01787. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
