

Validation of a risk stratification tool for fall-related injury in a state-wide cohort
- PMID: 28167743
- PMCID: PMC5293982
- DOI: 10.1136/bmjopen-2016-012189
Validation of a risk stratification tool for fall-related injury in a state-wide cohort
Abstract
Objective: A major preventable contributor to healthcare costs among older individuals is fall-related injury. We sought to validate a tool to stratify such risk based on readily available clinical data, including projected medication adverse effects, using state-wide medical claims data.
Design: Sociodemographic and clinical features were drawn from health claims paid in the state of Massachusetts for individuals aged 35-65 with a hospital admission for a period spanning January-December 2012. Previously developed logistic regression models of hospital readmission for fall-related injury were refit in a testing set including a randomly selected 70% of individuals, and examined in a training set comprised of the remaining 30%. Medications at admission were summarised based on reported adverse effect frequencies in published medication labelling.
Setting: The Massachusetts health system.
Participants: A total of 68 764 hospitalised individuals aged 35-65 years.
Primary measures: Hospital readmission for fall-related injury defined by claims code.
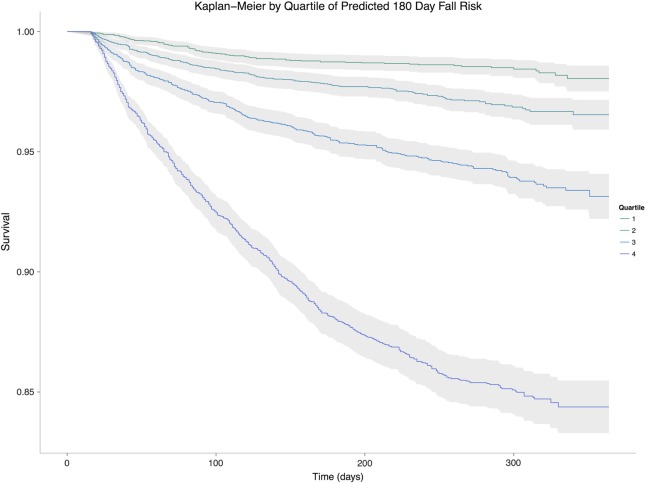
Results: A total of 2052 individuals (3.0%) were hospitalised for fall-related injury within 90 days of discharge, and 3391 (4.9%) within 180 days. After recalibrating the model in a training data set comprised of 48 136 individuals (70%), model discrimination in the remaining 30% test set yielded an area under the receiver operating characteristic curve (AUC) of 0.74 (95% CI 0.72 to 0.76). AUCs were similar across age decades (0.71 to 0.78) and sex (0.72 male, 0.76 female), and across most common diagnostic categories other than psychiatry. For individuals in the highest risk quartile, 11.4% experienced fall within 180 days versus 1.2% in the lowest risk quartile; 57.6% of falls occurred in the highest risk quartile.
Conclusions: This analysis of state-wide claims data demonstrates the feasibility of predicting fall-related injury requiring hospitalisation using readily available sociodemographic and clinical details. This translatable approach to stratification allows for identification of high-risk individuals in whom interventions are likely to be cost-effective.
Keywords: adverse effects; fall-related injury; health claims; precision medicine; prediction; risk stratification.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
All authors will complete the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that: THMJ, VMC, AC and AMR have read and understood BMJ policy on declaration of interests and declare that we have no competing interests. RHP has read and understood BMJ policy on declaration of interests and declares the following interests: RHP has served on advisory boards or provided consulting to Genomind, Healthrageous, Pamlab, Perfect Health, Pfizer, Psybrain and RIDVentures.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical