

Neuro-ophthalmological Complications of Chronic Inflammatory Demyelinating Polyradiculoneuropathy
- PMID: 28167978
- PMCID: PMC5291058
- DOI: 10.3109/01658107.2013.809459
Neuro-ophthalmological Complications of Chronic Inflammatory Demyelinating Polyradiculoneuropathy
Abstract
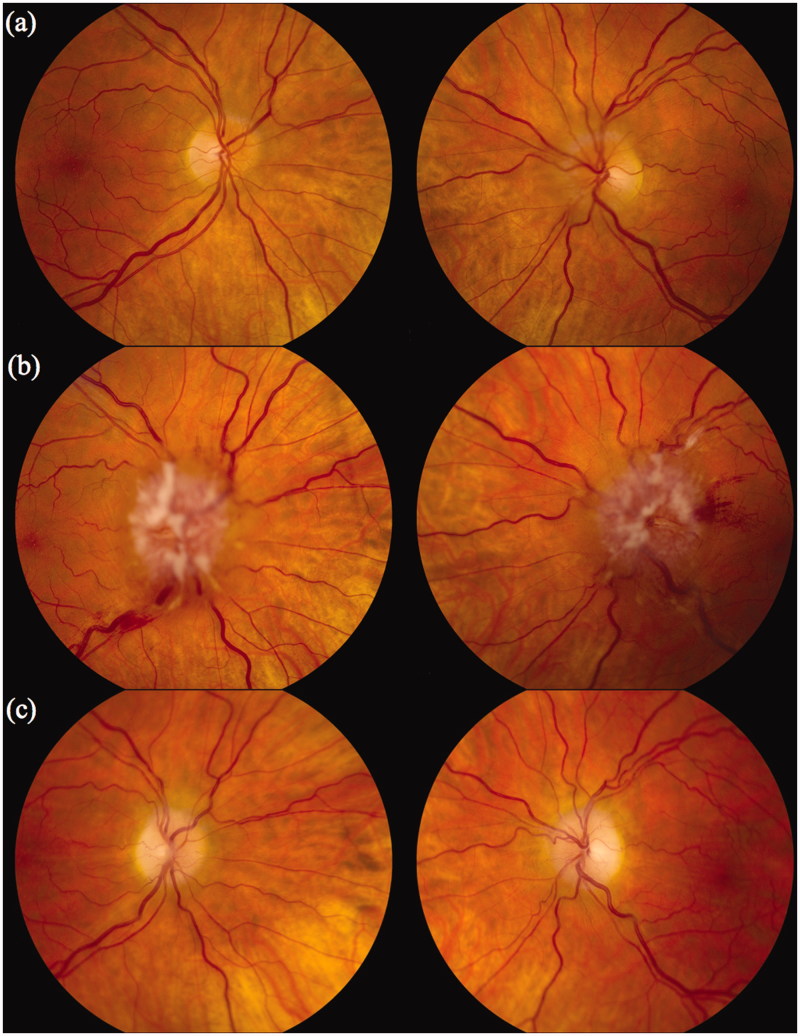
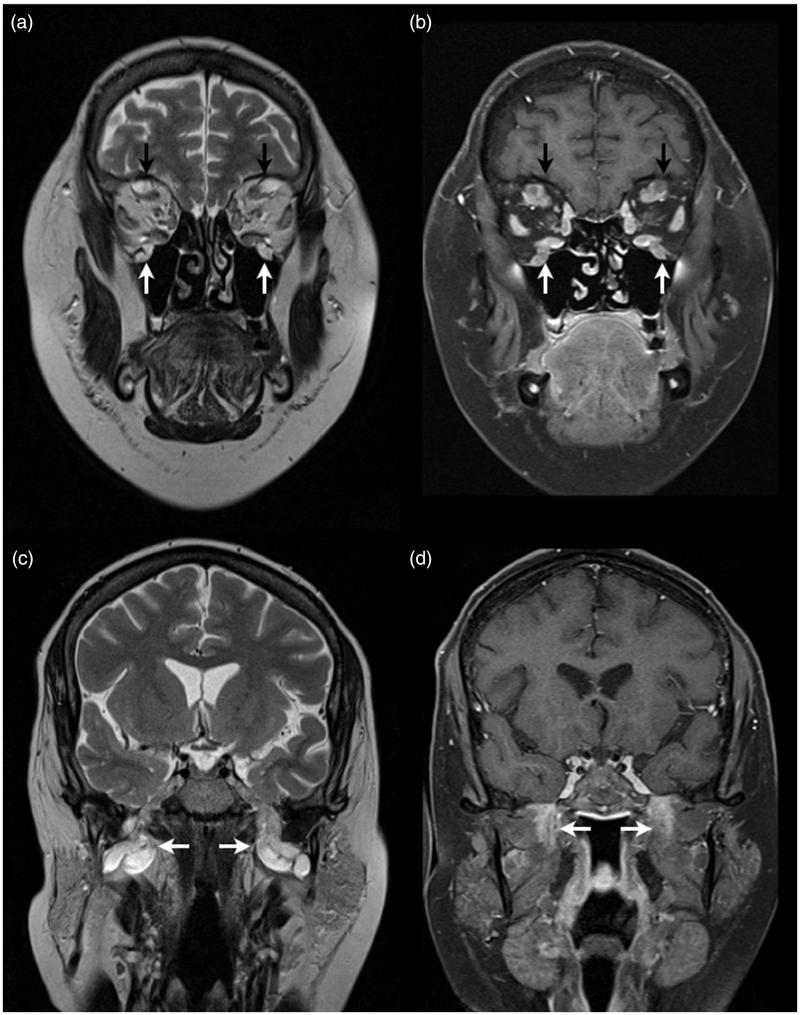
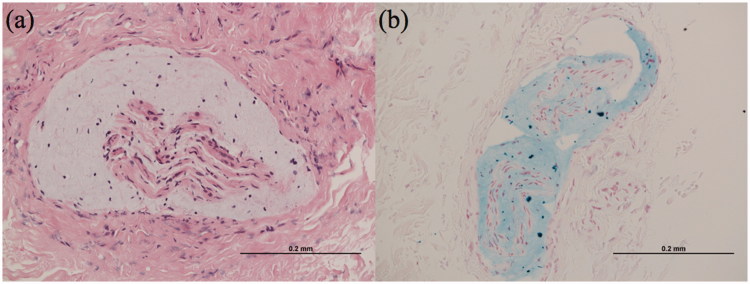
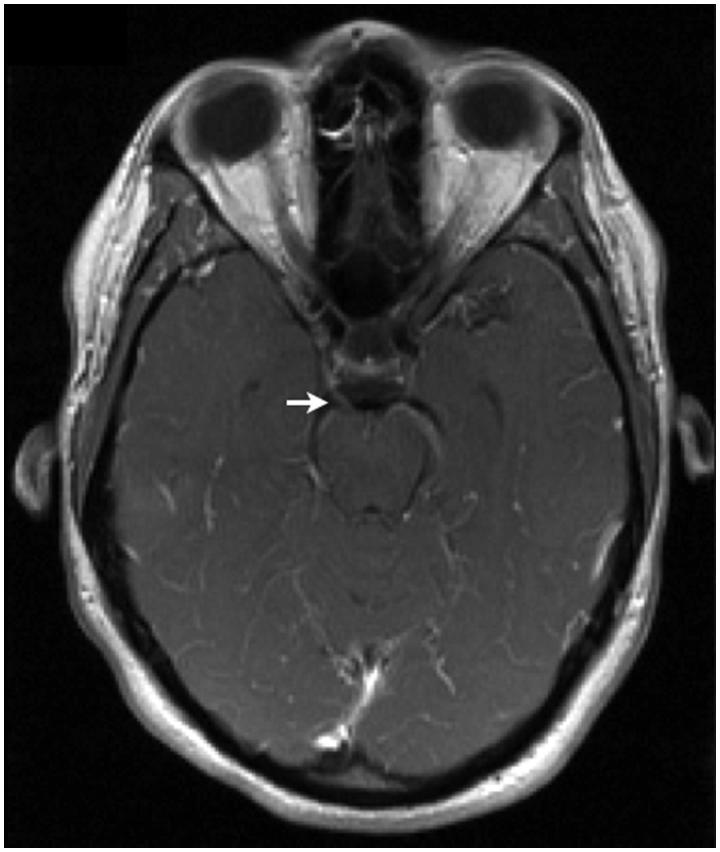
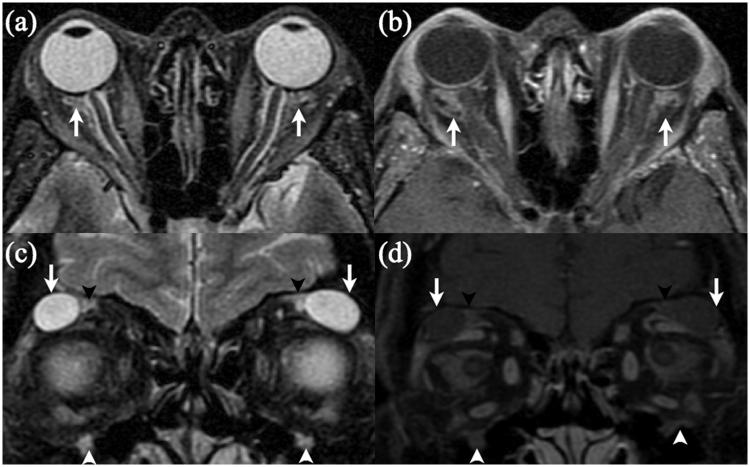
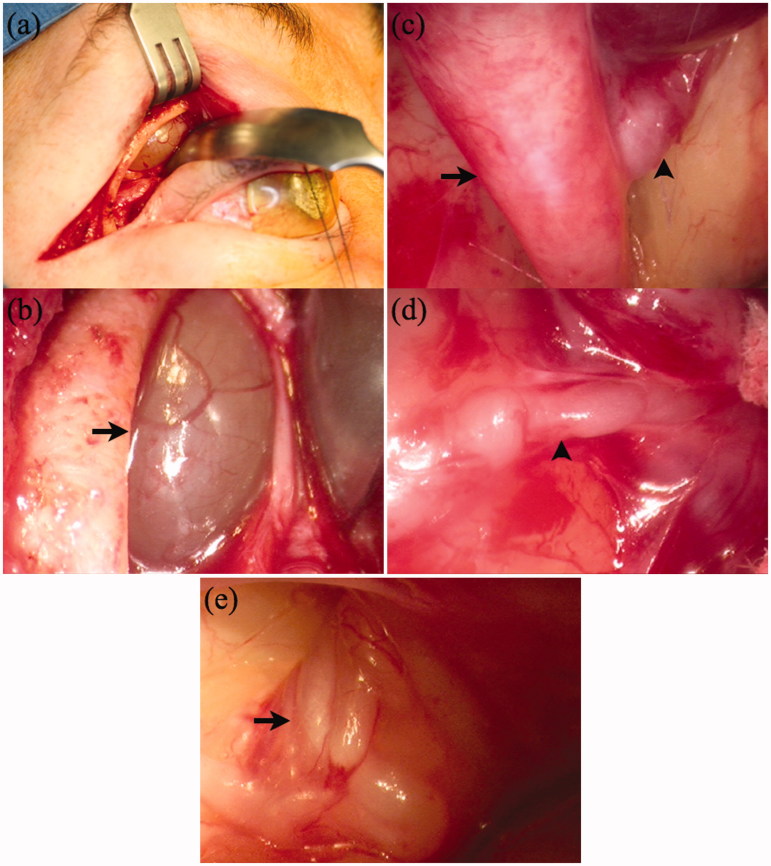
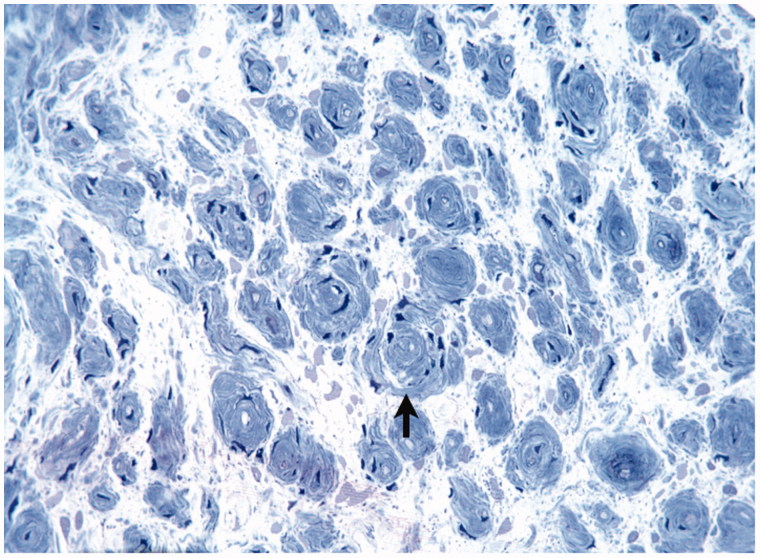
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) can lead to prominent nerve hypertrophy, which can mimic other forms of neuropathy radiologically. Neuro-ophthalmological complications can also occur in CIDP, either at presentation or chronically in the disorder. This can also cause diagnostic difficulties. We report three cases of neuro-ophthalmological complications of CIDP: two cases of papilloedema and one case of proptosis. In all three cases cranial nerve hypertrophy was present. CIDP should be considered in neuro-ophthalmological presentations associated with cranial/spinal nerve root hypertrophy.
Keywords: Chronic inflammatory demyelinating polyradiculoneuropathy; papilloedema; proptosis.
Figures
Similar articles
-
Extraocular Muscle Enlargement and Proptosis Associated with Chronic Inflammatory Demyelinating Polyradiculoneuropathy.Ophthalmic Plast Reconstr Surg. 2021 Sep-Oct 01;37(5):e176-e178. doi: 10.1097/IOP.0000000000001982. Ophthalmic Plast Reconstr Surg. 2021. PMID: 33795609
-
Ophthalmoplegia, proptosis, and lid retraction caused by cranial nerve hypertrophy in chronic inflammatory demyelinating polyradiculoneuropathy.J Neuroophthalmol. 2007 Jun;27(2):99-103. doi: 10.1097/WNO.0b013e318064c59b. J Neuroophthalmol. 2007. PMID: 17548992
-
[Chronic inflammatory demyelinating polyradiculoneuropathy associated with central nervous system involvement--as compared to multiple sclerosis].Rinsho Shinkeigaku. 1990 Sep;30(9):939-43. Rinsho Shinkeigaku. 1990. PMID: 2265502 Japanese.
-
The spectrum of acquired demyelinating polyradiculoneuropathy.Acta Neurol Belg. 1994;94(2):128-32. Acta Neurol Belg. 1994. PMID: 8036880 Review.
-
Chronic inflammatory demyelinating polyradiculoneuropathy and variants: where we are and where we should go.J Peripher Nerv Syst. 2014 Mar;19(1):2-13. doi: 10.1111/jns5.12053. J Peripher Nerv Syst. 2014. PMID: 24612201 Review.
Cited by
-
Chronic inflammatory demyelinating polyneuropathy: A unique case of chronic disease with atypical features.Radiol Case Rep. 2022 May 9;17(7):2441-2447. doi: 10.1016/j.radcr.2022.03.029. eCollection 2022 Jul. Radiol Case Rep. 2022. PMID: 35586159 Free PMC article.
-
CNS Involvement in Chronic Inflammatory Demyelinating Polyneuropathy: Subtle Retinal Changes in Optical Coherence Tomography.Neurol Neuroimmunol Neuroinflamm. 2021 Oct 19;9(1):e1099. doi: 10.1212/NXI.0000000000001099. Print 2022 Jan. Neurol Neuroimmunol Neuroinflamm. 2021. PMID: 34667130 Free PMC article.
-
A Case of Relapsing - Remitting CIDP with Sixth Nerve Palsy.Ann Indian Acad Neurol. 2021 Nov-Dec;24(6):939-941. doi: 10.4103/aian.AIAN_731_20. Epub 2021 Oct 11. Ann Indian Acad Neurol. 2021. PMID: 35359551 Free PMC article. No abstract available.
-
Primary and Secondary Optic Nerve Sheath Meningioma.J Neurol Surg B Skull Base. 2021 Feb;82(1):27-71. doi: 10.1055/s-0041-1723801. Epub 2021 Feb 18. J Neurol Surg B Skull Base. 2021. PMID: 33777618 Free PMC article.
-
An Atypical Phenotype of Chronic Inflammatory Demyelinating Polyradiculoneuropathy Associated with Ocular Palsy, IgM-anti Ganglioside Antibody, and Fever-induced Recurrence.Intern Med. 2022 Apr 15;61(8):1247-1252. doi: 10.2169/internalmedicine.7526-21. Epub 2021 Oct 5. Intern Med. 2022. PMID: 34615817 Free PMC article.
References
-
- Joint Task Force of the EFNS and the PNS Federation of Neurological Societies/Peripheral Nerve Society guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society. J Peripher Nerv Syst 2005;10:220–228 - PubMed
-
- Tackenberg B, Lunemann JD, Steinbrecher A, Rothenfusser-Korber E, Sailer M, Brück W, Schock S, Zschenderlein R, Zipp F, Sommer N. Classifications and treatment responses in chronic immune-mediated demyelinating polyneuropathy. Neurology 2007;68:1622–1629 - PubMed
-
- Lunn MPT, Willison HJ. Diagnosis and treatment in inflammatory neuropathies. J Neurol Neurosurg Psychiatry 2009;80:249–258 - PubMed
-
- Duggins AJ, McLeod JG, Pollard JD, Davies L, Yang F, Thompson EO, Soper JR. Spinal root and plexus hypertrophy in chronic inflammatory demyelinating polyneuropathy. Brain 1999;122:1383–1390 - PubMed
-
- Niino M, Tsuji S, Tashiro K. Chronic inflammatory demyelinating polyneuropathy with multiple hypertrophic nerves in intracranial, and intra- and extra-spinal segments. Int Med 1999;38:445–449 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources